Measuring ROI on Longevity Interventions
Return on investment sounds clean until the underlying asset is extra healthy life. Longevity medicine still attracts the wrong scoreboard. Readers are asked to treat a shifted biomarker, a lower inflammatory marker, or a younger-looking clock as if it were equivalent to more years of preserved function. It is not. The real return has to be measured through outcome quality, time horizon, adherence burden, and how much uncertainty still sits between the intervention and lived health.
What Counts as Return in Longevity
That distinction matters because longevity claims are often sold through immediacy while true payoffs are deferred. A reader can observe a lab change next month. They cannot directly observe whether that change means fewer years with frailty, lower dementia risk, or more disability-free time three decades later. The absence of a short feedback loop invites overclaiming.
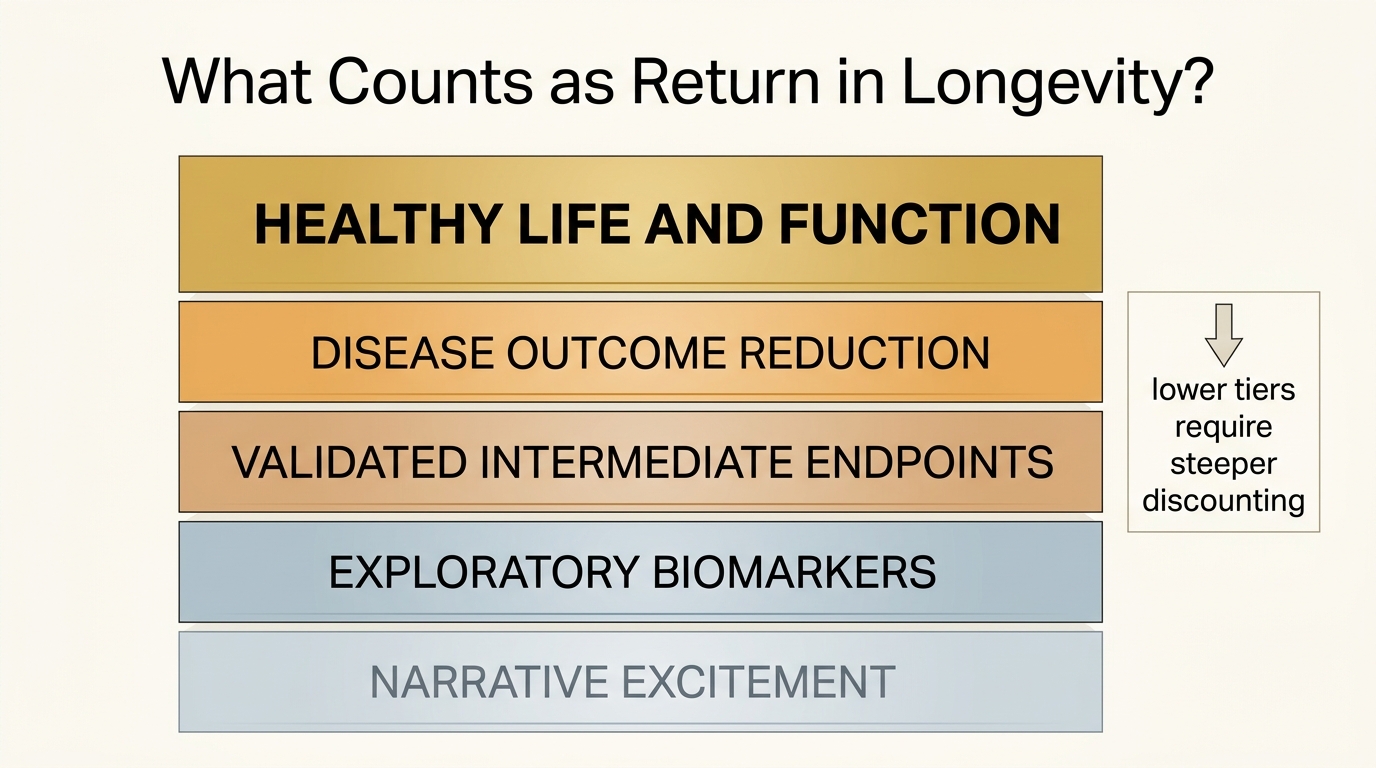
The correct frame is to separate return layers. At the top sit hard outcomes such as survival, disability-free years, and preserved function. Below that sit disease-specific risk reductions. Below that sit validated intermediate endpoints. Below that sit exploratory biomarkers and model outputs. The lower the layer, the more discount rate should be applied to any ROI claim.
Established fact: geroscience trials still face unresolved endpoint and surrogate-validation problems, which means biomarker movement alone cannot be treated as proof of healthy-life gain. Reasoned inference: the practical ROI of most current longevity interventions is highest when they improve risk factors or function that already have known clinical meaning, and lowest when they rely mainly on narrative extrapolation from exploratory signals.
Healthy Life Beats Raw Lifespan
The next mistake is to talk as if extra years and better years are interchangeable. They are not. A return metric that ignores healthy life expectancy can reward the wrong intervention mix. An intervention that delays one disease marker but does little for multi-system function may look attractive on paper while doing very little for the life readers actually want to preserve.
This is why compression of morbidity remains one of the most useful lenses in the field. The highest-value return is not merely adding time after multiple systems have already failed. It is preserving autonomy, mobility, cognition, and resilience while compressing the years spent in high-burden decline.
Biomarkers Are Inputs, Not Payouts
Biomarkers matter because they can show target engagement and help stratify risk. They do not become return by themselves. A clock age shift, a glucose improvement, or a lower apoB can be highly useful. Each still needs interpretation. Does it map to a pathway with known clinical consequence? Is the measurement stable? Is the benefit likely to persist under long-run adherence? How much downside or opportunity cost was required to produce it?
That is why readers should pair this topic with Biological Age Clocks as Decision Tools and Off-Label Longevity Prescriptions: Risks and Patterns. Both pieces make the same point from different angles: measurement can inform judgment, but it does not replace outcome discipline.
Time Horizon Changes the Math
Longevity ROI is unusually sensitive to time. A low-cost intervention with modest annual benefit can outrun a dramatic but unproven protocol if the modest intervention is sustainable for years and anchored to known risk reduction. The reverse can also happen. An expensive frontier therapy can look exciting but produce negative real return once uncertainty, retreatment frequency, and unresolved side effects are priced honestly.
Age and baseline risk change the equation further. An intervention that plausibly lowers future cardiometabolic damage may have much higher expected payoff in a reader with clear metabolic dysfunction than in a low-risk reader already near the floor of preventable burden. The same molecule therefore has different expected return depending on starting state, not only on its mechanism.
Cost, Friction, and Adherence Are Part of the Return
Financial cost is only one drag. Intervention friction matters too. A protocol with heavy scheduling burden, persistent side effects, or nutritional tradeoffs can erode its own return even if it nudges a biomarker in the right direction. Readers do not live inside trial protocols. They live inside routines, appetite, sleep debt, family obligations, and limited willingness to maintain complexity for decades.
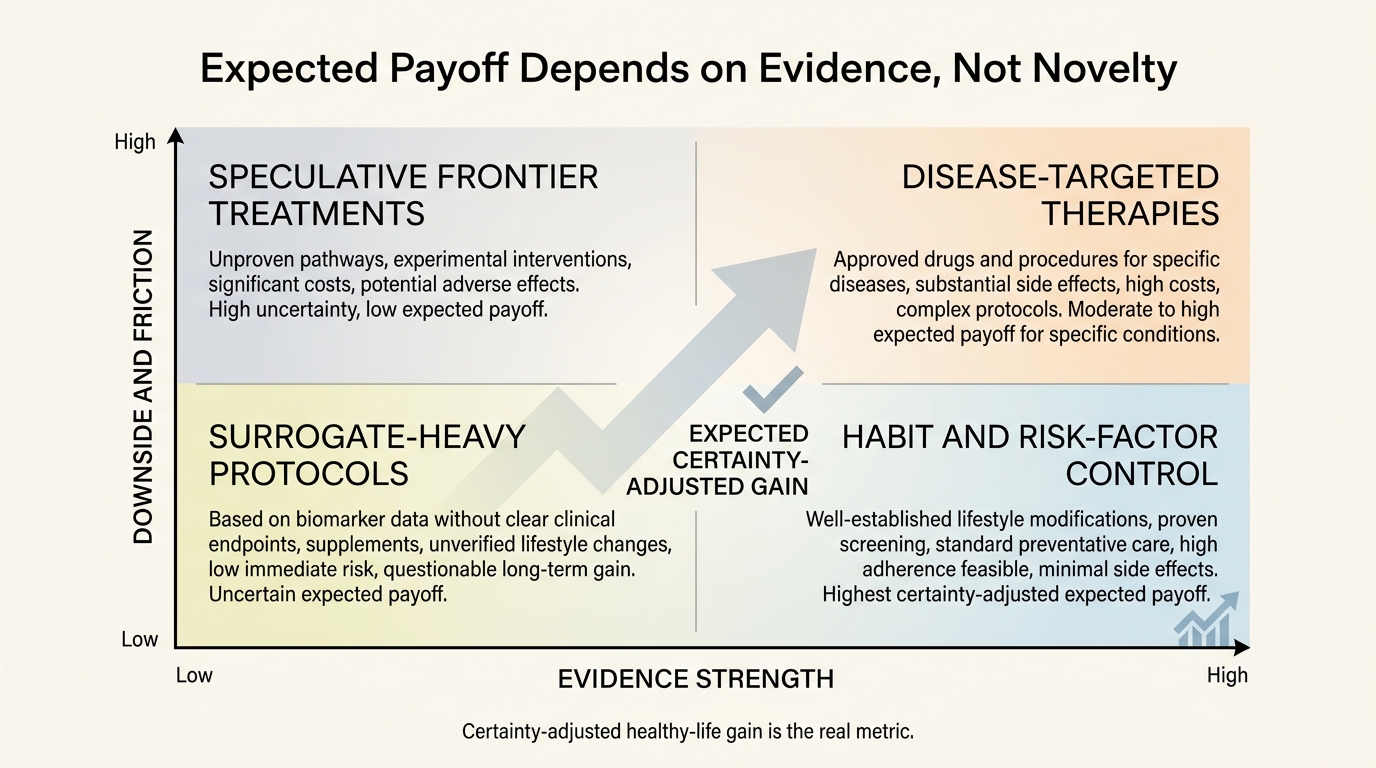
That makes the highest-ROI interventions look less glamorous than the market prefers. Sleep discipline, blood-pressure control, lipid management, exercise, weight normalization where needed, and carefully chosen disease-targeted therapies often have clearer real-world return than boutique protocols built on thin surrogate stacks. This is not because frontier science is fake. It is because ROI should reward certainty-adjusted healthy-life gain, not novelty premium.
| Return layer | What it captures | Main failure mode |
|---|---|---|
| Healthy-life and function endpoints | Autonomy, disability-free time, preserved cognition and mobility | Slow feedback and expensive trials |
| Disease-specific outcome reduction | Lower event risk in clinically legible domains | May not generalize to whole-body aging |
| Validated intermediate markers | Risk-factor improvement with known clinical meaning | Overstating whole-life impact from one pathway |
| Exploratory biomarkers and clocks | Target engagement, stratification, trend detection | Confusing measurement movement with durable payoff |
Decision-Grade Take for Readers
The correct question is not “Did the intervention do something?” Almost all interventions do something. The right question is “What is the expected healthy-life value of what it did, after discounting for uncertainty, cost, downside, and adherence?” Once framed that way, much of the longevity market reprices downward, and a smaller set of interventions begins to look genuinely compelling.
- Use healthy life and function as the top ROI endpoints whenever possible.
- Discount biomarker-only claims unless the biomarker sits on a pathway with known clinical consequence.
- Price time horizon, adherence burden, and side effects into every longevity claim.
- Prefer certainty-adjusted gains over novelty-adjusted storytelling.
Known, Inferred, and Unknown
| Category | Assessment |
|---|---|
| Known | Healthy life expectancy and total life expectancy are related but distinct endpoints, and gains in one do not automatically match gains in the other. |
| Known | Geroscience trials still lack fully validated surrogate endpoints that can stand in cleanly for broad anti-aging benefit. |
| Known | Biomarkers can support stratification and target engagement without proving durable clinical payoff. |
| Inferred | The highest real-world ROI for most readers still comes from interventions that improve established risk factors or function with tolerable long-run friction. |
| Unknown | Which current aging biomarkers, if any, will become trusted surrogate endpoints for broad healthy-life gain across multiple intervention classes. |
Source Frame
This article uses the WHO Global Health Observatory page on life expectancy and healthy life expectancy for the distinction between living longer and living longer in good health.
For endpoint-selection constraints in geroscience trials, it uses Endpoints for geroscience clinical trials: health outcomes, biomarkers, and biologic age and Selecting Appropriate Clinical Trial Endpoints for Geroscience Trials: A Path Towards Consensus.
For biomarker selection logic, it uses the TAME workgroup framework A framework for selection of blood-based biomarkers for geroscience-guided clinical trials. For the regulatory meaning of surrogate endpoints, it uses the FDA page Surrogate Endpoint Resources for Drug and Biologic Development. The unresolved issue is not whether biomarkers help. It is how many of them will earn the right to be treated as payout rather than as signal.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.