Oral GLP-1 Enters Phase 3 Reality: Convenience, Adherence, and Longevity Tradeoffs
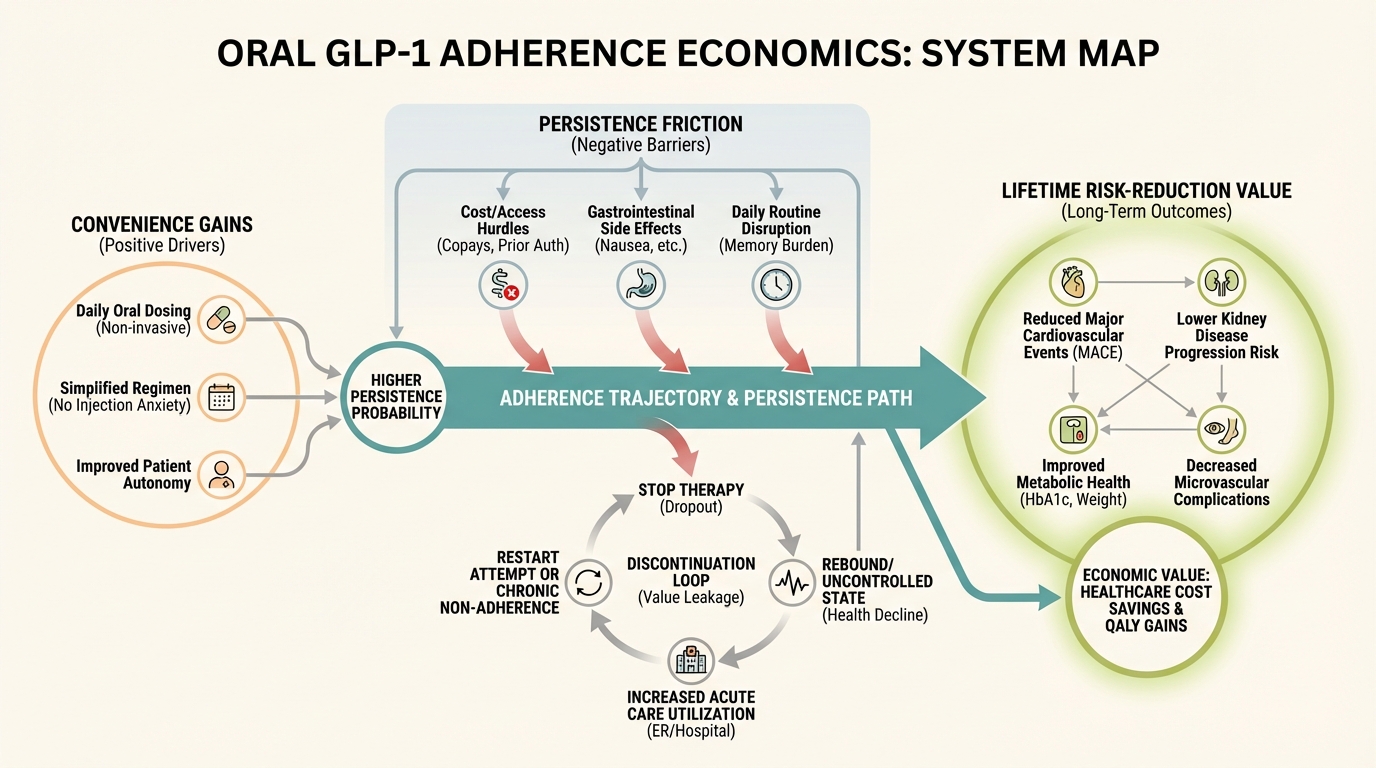
Oral GLP-1 is not only a formulation shift. It is a delivery-system shift that changes persistence, access, and long-horizon risk reduction economics.
ATTAIN-era phase 3 results moved oral GLP-1 from a speculative branch into a practical operating question for clinicians and households: does easier administration improve durable adherence enough to produce better lifetime outcomes? The answer is not automatic. Convenience can improve uptake, but persistence still depends on tolerability, affordability, expectation setting, and protocol quality.
Core thesis: oral GLP-1 expands the addressable adherence envelope, but longevity-relevant benefit still depends on persistence architecture, not initiation alone.
Why Delivery Form Matters
Injection aversion, routine friction, and administration burden suppress persistence in many real-world pathways. Oral administration can remove one barrier, but it introduces others such as timing discipline, gastrointestinal tolerability management, and potentially faster restart-stop cycling if counseling is weak.
The durability question therefore becomes behavioral and operational, not purely pharmacologic.
Phase 3 Signal and Interpretation Boundaries
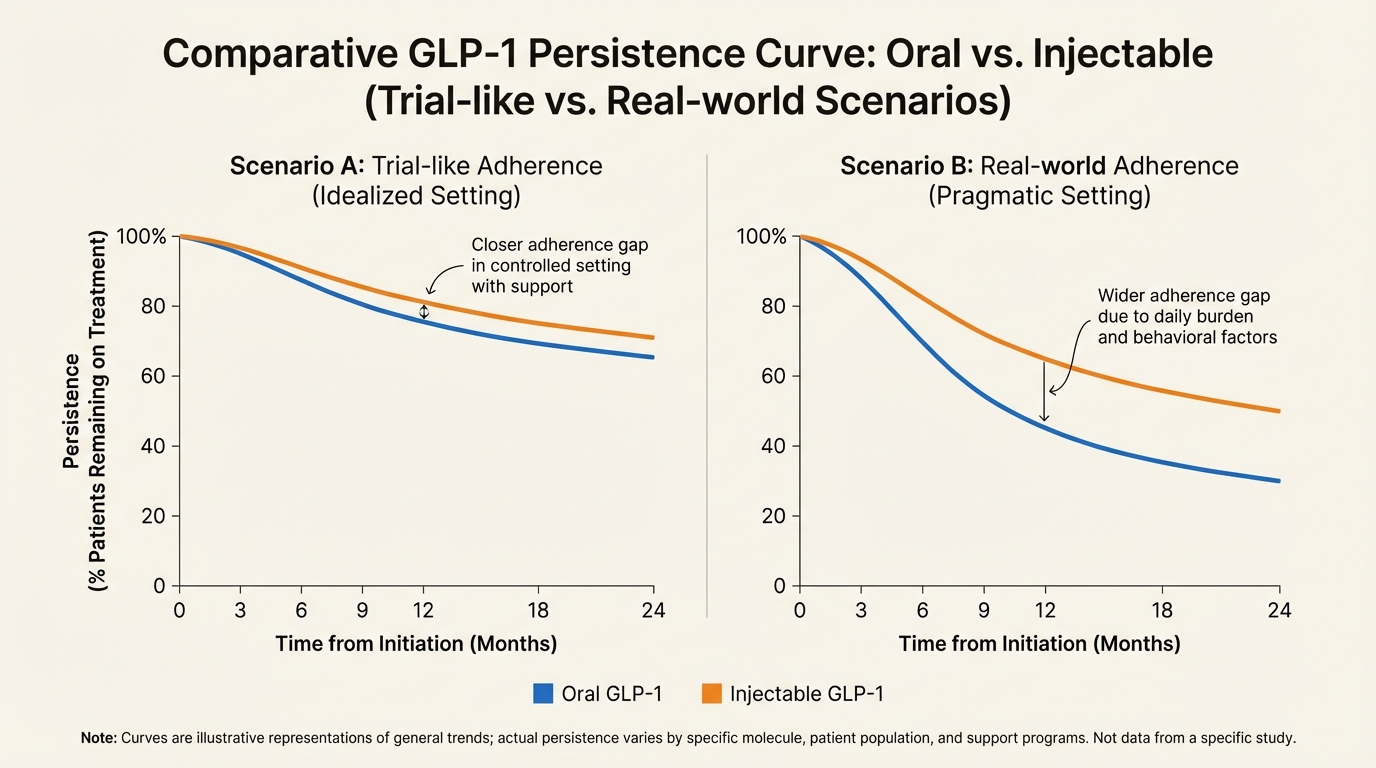
Phase 3 efficacy signal can be strong while long-run persistence remains uncertain. Trial conditions include structured follow-up, standardized counseling, and selective populations. Real-world settings are noisier. This is why clinics should track persistence curves and dose-maintenance intervals explicitly rather than assuming trial completion rates will transfer directly.
The Discontinuation Problem
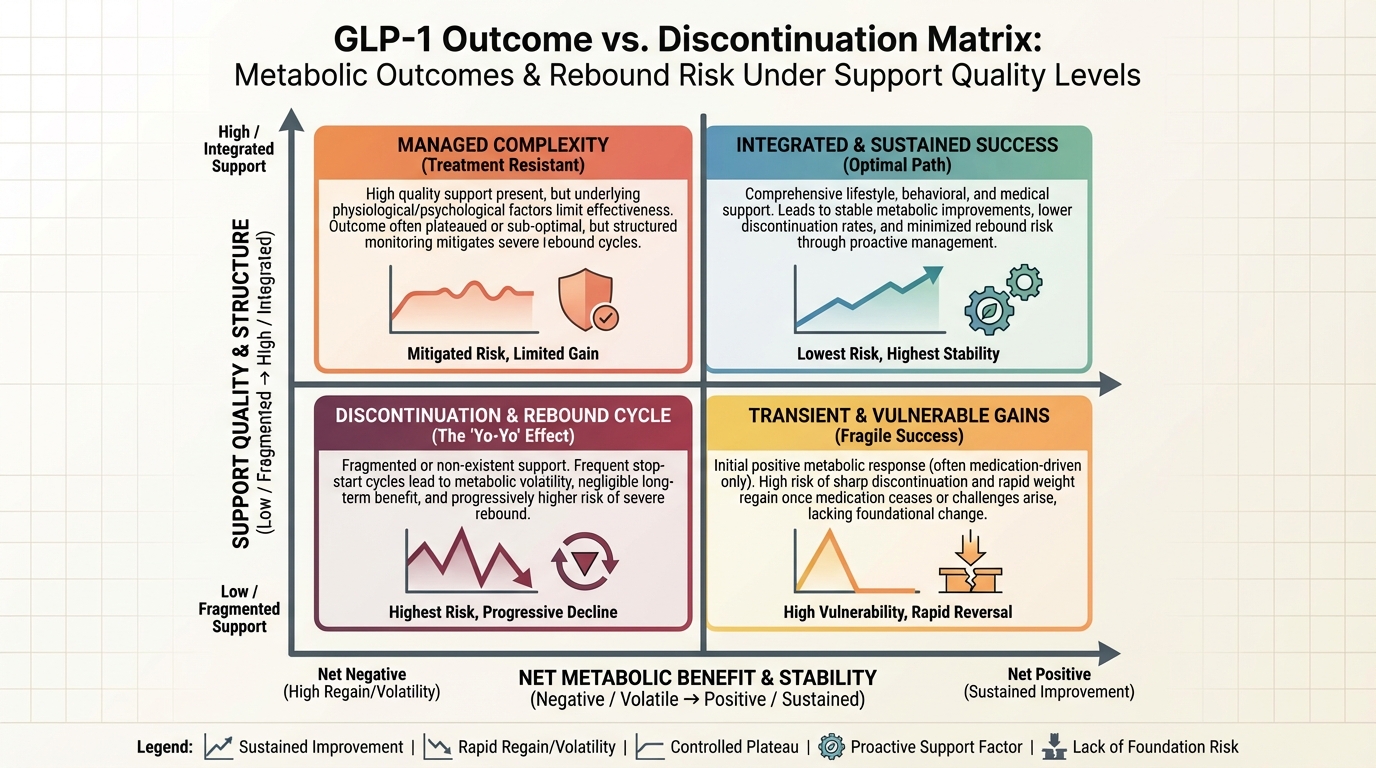
Many households experience this sequence: rapid early improvement, expectation overshoot, side-effect fatigue, discontinuation, and partial rebound. If this cycle is not addressed up front, cost effectiveness degrades and confidence in preventive care drops. The correct response is proactive cycle-breaking design with side-effect coaching, dose cadence review, nutrition-protein planning, and strength-preserving activity.
Long-Horizon Cost and Access
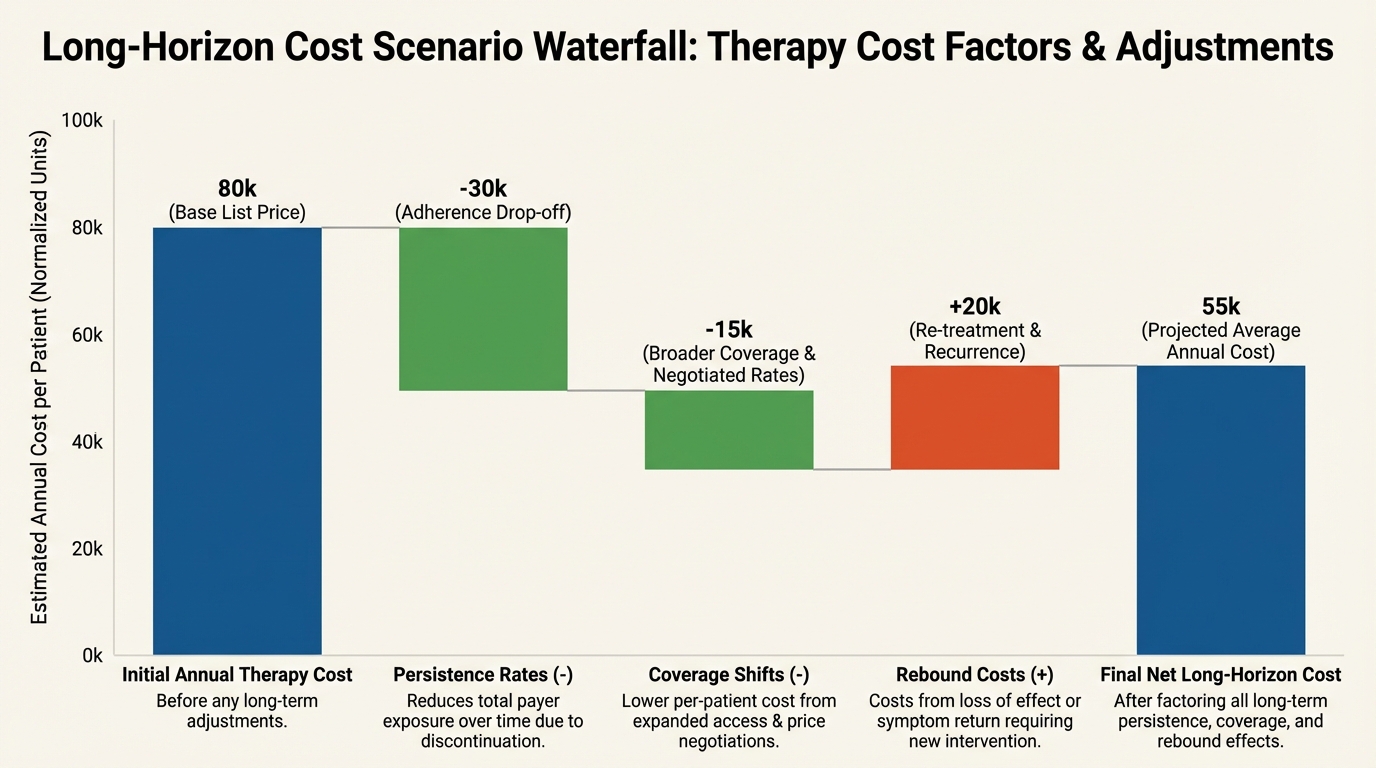
Convenience without affordability does not scale population benefit. Oral options could improve competitive pricing over time, but current planning should still use conservative cost scenarios and include fallback pathways. The operational question for households is not only whether therapy works, but whether it is sustainable for the planned risk window.
Operational Bottom Line
Oral GLP-1 can be a major access and adherence upgrade. It is not self-executing. The clinical winner is the program that treats adherence as a designed system, tracks persistence as a core metric, and protects functional outcomes while targeting metabolic risk.
Source List
Orforglipron phase 3 update: Eli Lilly ATTAIN-2 release.
ATTAIN-2 publication record: PubMed 41275875.
Regulatory obesity and diabetes context: FDA drug safety context.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.