AI-Accelerated Drug Discovery in Aging: Real Compression, Real Bottlenecks
AI is accelerating the throughput of longevity discovery. It does not remove the need for biological validation, regulatory rigor, or durable clinical outcomes.
Two claims currently coexist in longevity discourse. The first states AI has transformed the search for anti-aging interventions. The second states the clinic moves at a different speed. Both are true. Readers must separate discovery acceleration from patient-level evidence. Missing this distinction distorts timelines and fragilizes portfolio decisions.
What Is Established
AI materially improves upstream discovery throughput
Modern models support target ranking, protein structure prediction, and molecule prioritization at a scale previously unfeasible in traditional workflows. DeepMind and Isomorphic Labs reported AlphaFold 3 performance improvements in biomolecular structure prediction, expanding the utility of model-guided hypothesis generation for drug design. OpenAI and Retro Biosciences have framed their collaboration around similar acceleration dynamics in life-science workflows. These tools enable researchers to simulate interactions across vast chemical libraries and biological targets, reducing reliance on costly, time-consuming brute-force screening. However, computational efficiency gains are most pronounced in silico and require careful calibration to real-world biological variability.
Senolytic screening now demonstrates a concrete AI use case
In senolytic discovery, AI-assisted pipelines evaluate large molecular sets to identify selective candidates for experimental follow-up. Published work shows machine-learning ranking reduces the wet-lab search burden and increases hit quality. The implication is specific: fewer blind screens and better candidate prioritization. This does not guarantee clinical success. For instance, recent studies using convolutional neural networks and graph-based models predicted senolytic activity with higher precision than traditional methods. Yet, these candidates still face rigorous in vitro and in vivo validation to confirm specificity and minimize off-target effects.
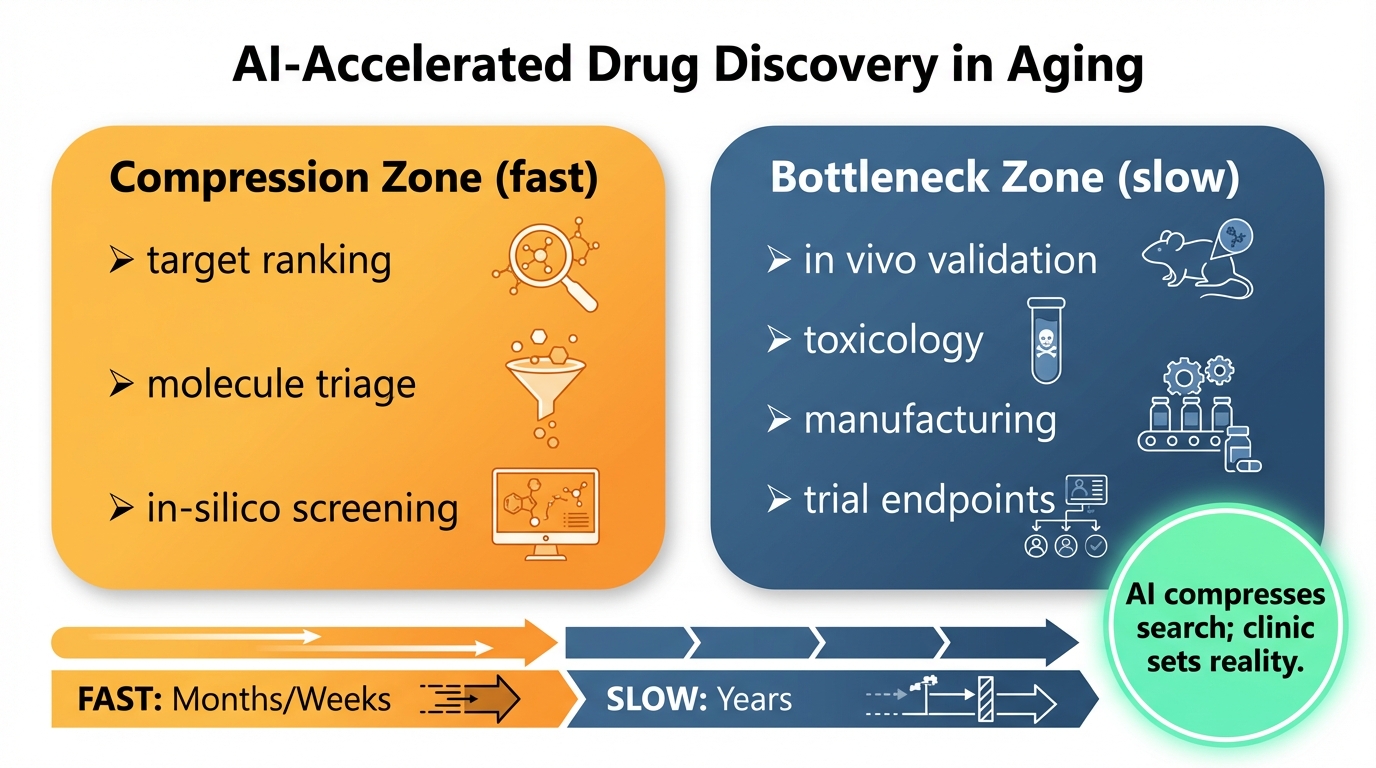
Discovery acceleration is measurable before clinical approval
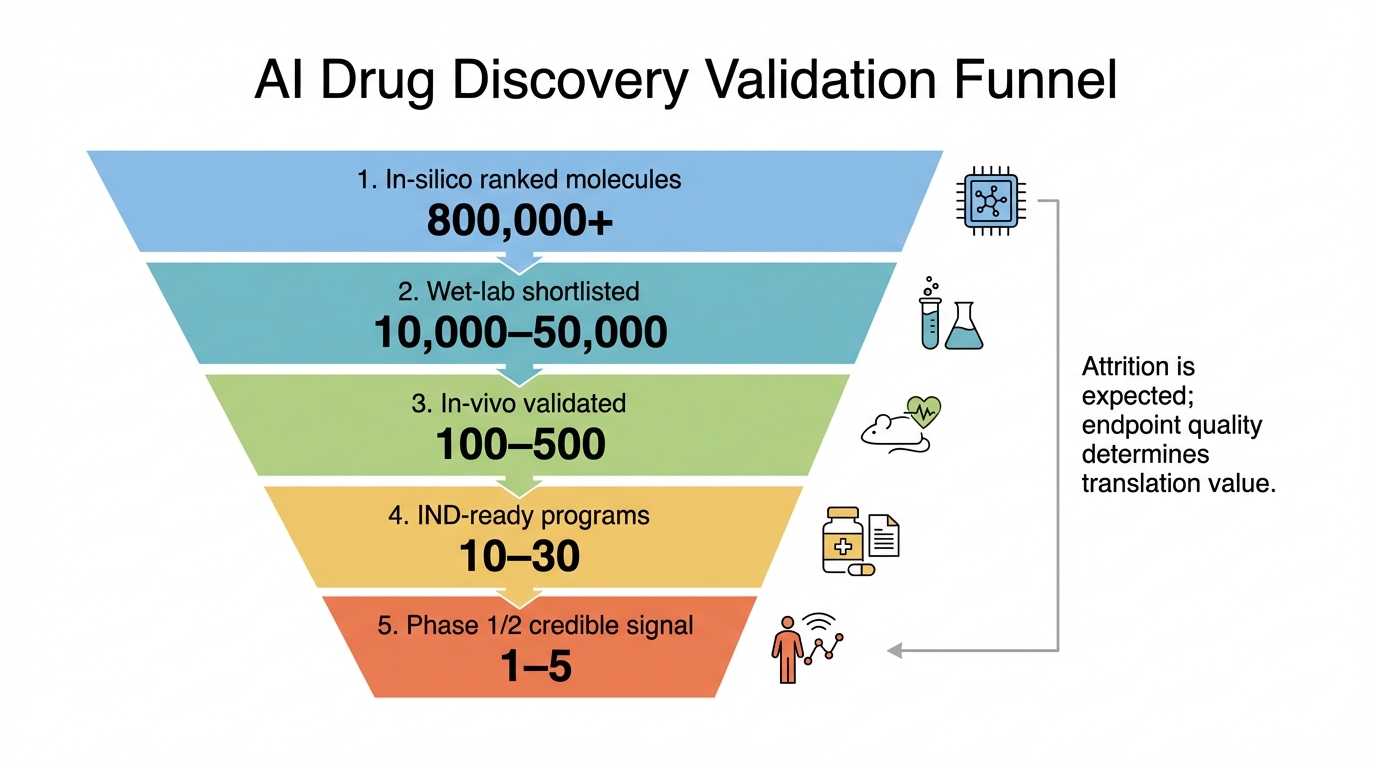
The greatest time savings occur at the top of the funnel. Candidate generation, triage, and early prioritization now run with higher throughput. The bottom of the funnel remains constrained by animal validation, pharmacokinetics, toxicology, manufacturing quality, trial recruitment, endpoint selection, and long follow-up. This asymmetry explains why scientific momentum feels rapid while approved interventions remain sparse. Metrics such as reduced time-to-lead and increased preclinical hit rates are tangible. However, they do not directly translate to shortened regulatory review or faster market entry without concurrent improvements in translational science.
Where The Field Is Still Vulnerable
Overfitting to proxy objectives
Models may optimize for tractable proxy labels that fail to capture real biological complexity in humans. A high in-silico score does not guarantee acceptable efficacy-to-safety tradeoffs in vivo. Aging biology heightens this risk because many pathways are context-sensitive across tissues and disease states. For example, a compound predicted to enhance autophagy in cell lines may exhibit pleiotropic effects in whole organisms, where cross-talk between systems and age-related comorbidities alter drug response. Rigorous multi-omics validation and cross-species consistency checks are necessary to mitigate over-optimistic projections from narrow computational assessments.
Dataset and assay mismatch
Training data often derives from heterogeneous assays with inconsistent endpoints. If assay conditions and target definitions are not harmonized, model confidence can exceed evidence quality. Result quality reflects curation quality as much as algorithm design. Discrepancies in experimental protocols, cell lines, or measurement techniques introduce noise that machine learning models may inadvertently learn, reducing generalizability. Standardization efforts and meta-analyses are critical to align data sources, but these are resource-intensive and lag behind model development, creating a persistent gap between computational output and biological reality.
Translation bottlenecks are not optional
Regulators and clinicians still require reproducible safety and patient-relevant outcomes. High throughput increases candidate volume, but without stronger translational design, it can also increase downstream attrition and capital burn. Translating bench to bedside involves phases where AI offers limited assistance, such as designing adaptive clinical trials, establishing biomarkers with clinical utility, and navigating regulatory frameworks tailored to novel aging endpoints. Investments in integrated platforms bridging computational discovery with translational research are essential to convert accelerated candidate generation into viable therapeutic pipelines.
Evidence Map For Decision-Makers
Known: AI improves speed and scale in target and molecule prioritization.
Inferred: Better prioritization should improve R&D capital efficiency over time.
Unknown: The magnitude and timing of patient-level outcome gains in broad aging indications.
This evidence map matters for scientific expectations and public communication. Judging AI progress solely by final approvals underestimates current progress. Judging it solely by ranking speed and early hits ignores clinical difficulty. A high-fidelity interpretation needs both layers. Decision-makers should track intermediate metrics like reduced preclinical cycle times and improved candidate quality, while maintaining realistic timelines for clinical validation and regulatory milestones.
How To Read New Claims Correctly
Identify where in the funnel the claim sits
Claims about target discovery, molecule ranking, or preclinical signals should not be interpreted as equivalent to validated patient benefit. Such claims remain meaningful, but only at their actual evidence layer. For instance, an announcement of novel target identification via AI warrants scrutiny of biological plausibility and prior art, not immediate extrapolation to therapeutic impact. Contextualizing claims within the drug development pipeline prevents misallocation of attention and resources.
Check whether independent teams reproduce directionality
A single pipeline may show promising results for reasons that do not transfer. Replication across teams, assays, and models is a stronger marker of durable progress than isolated performance highlights. Cross-validation through public-private partnerships, shared benchmarking datasets, and open-source tooling helps distinguish robust advances from method-specific artifacts. Consistency in findings across diverse research groups indicates generalizability and reduces the risk of overfitting to localized data or algorithmic idiosyncrasies.
Track endpoint quality in ongoing programs
Longevity interventions that reach practice will pair mechanistic plausibility with clinical outcomes and acceptable safety. Programs relying on narrative velocity without endpoint depth will not build durable credibility. Scrutinize trial designs for clinically relevant endpoints, such as functional improvement or disease modification, rather than surrogate markers alone. Programs demonstrating progressive validation from cellular models to animal studies and early human trials with clear efficacy signals are more likely to succeed and deserve prioritized attention.
What This Means For LEV Framing
AI acceleration strengthens the case that discovery cycles are entering a compounding phase. It does not remove translational bottlenecks. The most defensible LEV interpretation in 2026 is that enabling technologies are converging, while clinical validation and scalable access remain central constraints. The convergence of AI with CRISPR, senolytics, and other platform technologies suggests an expanding toolkit for intervention discovery. Yet, the path to widespread clinical adoption depends on overcoming biological complexity and regulatory hurdles.
The practical takeaway is disciplined optimism. Progress is real. Extrapolation still needs guardrails. Stakeholders should balance enthusiasm for technological advances with investments in translational infrastructure, regulatory science, and robust clinical trial networks to ensure accelerated discovery translates into tangible healthspan extension.
Source List
Abramson, J., et al. (2024). Accurate structure prediction of biomolecular interactions with AlphaFold 3. Nature.
OpenAI. (2026). Accelerating life sciences research with Retro Biosciences.
Nature Aging. (2024). Discovery and synthesis of novel senolytics using deep neural network modeling.
Gomes, B., et al. (2023). Machine learning identifies compounds with senolytic activity against senescent cells. Nature Aging.
Nature Biotechnology. (2025). When does anti-ageing become medicine? (Translational context).