GLP-1 Drugs as Potential Longevity Agents
GLP-1 class therapies are now the most credible near-term bridge between metabolic medicine and longevity medicine. This bridge is real, but it fails if function is not protected.
Longevity medicine often focuses on future platform technologies. GLP-1 and dual incretin therapies demand a different approach: a therapy can be available now, produce strong disease-modifying effects in high-burden populations, and still require disciplined execution to avoid long-term tradeoffs. This is why the current question is not “Do GLP-1 drugs work?” The question is “Under what protocol do they improve lifespan-relevant outcomes without increasing frailty risk?” Success depends on maintaining physiological resilience while achieving metabolic correction. Clinicians must balance efficacy against functional preservation.
What Is Established
Cardiometabolic benefits are now substantial
Semaglutide has demonstrated clinically meaningful cardiovascular event reduction in patients with overweight or obesity and established cardiovascular disease. Kidney outcome data in type 2 diabetes and chronic kidney disease also strengthened the case that GLP-1 class therapies may influence multiple age-related disease pathways rather than isolated weight metrics. These findings suggest effects beyond glucose control, including anti-inflammatory properties and improved endothelial function that collectively contribute to reduced morbidity in aging populations.
The class has moved beyond obesity branding
The evidence profile now includes obesity, glycemic control, cardiovascular risk, and renal outcomes. This multi-domain effect pattern is a core reason commentators increasingly discuss GLP-1s in longevity terms. The framing is justified when endpoint quality is retained. It becomes weak when discussion collapses into cosmetic weight narratives. Moving from weight-centric to healthspan-focused evaluation marks a maturation in clinical understanding and application, positioning these agents as multidimensional interventions rather than singular metabolic tools.
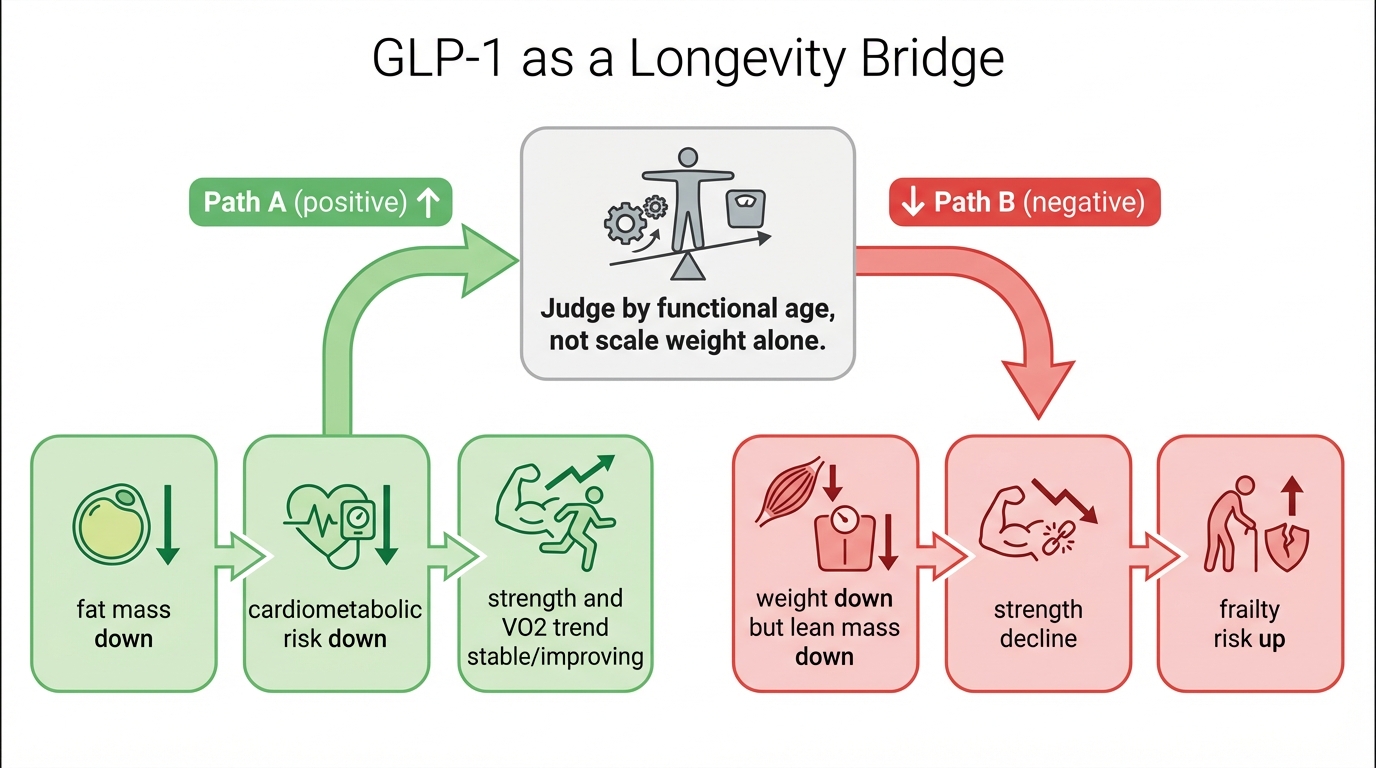
Functional downside risk is real
Loss of lean mass during rapid weight loss is a key implementation risk. If strength and aerobic capacity decline while scale weight improves, functional age can worsen. That outcome is avoidable but not automatic. It requires protocol design, not hope. Losing metabolically active tissue can paradoxically increase long-term mortality risk despite improved metabolic parameters. This paradoxical risk demands careful management through structured intervention protocols.
What Still Needs Better Data
Long-duration frailty and disability trajectories
The next evidence layer is not short-term body composition alone. It is long-term function: strength preservation, mobility, falls risk, hospitalization burden, and independence metrics in older cohorts and comorbidity-heavy populations. Current trials typically focus on 1-2 year outcomes, while longevity-relevant effects require decade-scale observation to assess true impact on healthspan extension and disability-free survival rates across diverse demographic groups.
Best-practice co-intervention protocols
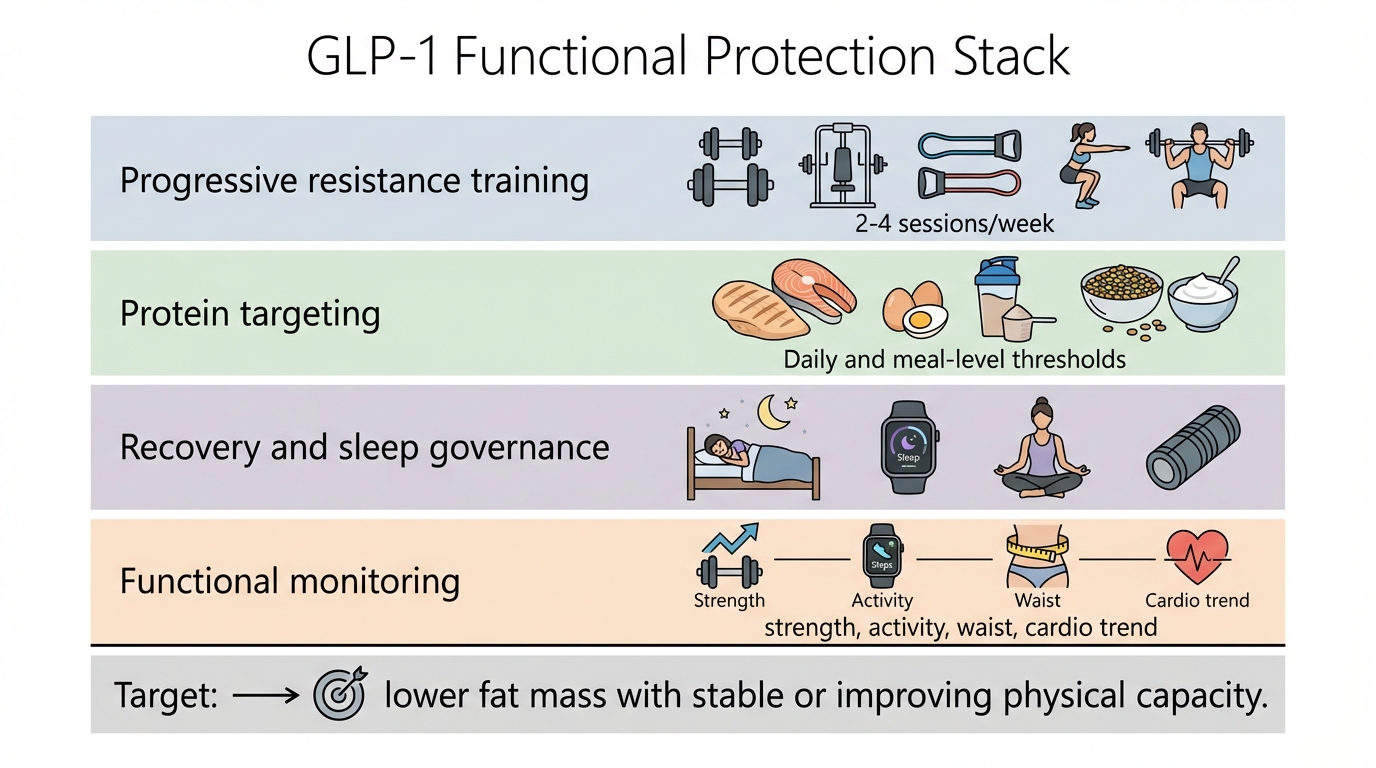
Clinical practice still varies in how aggressively programs pair GLP-1 therapy with resistance training, nutrition targets, and recovery design. More standardized implementation studies would reduce avoidable heterogeneity in outcomes. Optimal protein intake thresholds, exercise prescription specificity, and micronutrient supplementation strategies remain inadequately defined for patients undergoing significant metabolic transformation. These gaps affect real-world efficacy.
Durability under real-world adherence constraints
Lifecycle management matters. Medication access, adherence persistence, cost, and behavioral support determine whether early gains persist or reverse. The transition from clinical trial conditions to routine practice introduces numerous variables affecting long-term sustainability, including socioeconomic factors, healthcare system support structures, and individual psychological adaptation to chronic therapy requirements.
Practical Clinical Hierarchy
Tier 1 outcomes: cardiovascular and renal events, mortality-relevant disease burden.
Tier 2 outcomes: body composition plus physical capacity trajectory.
Tier 3 outcomes: scale weight and short-term aesthetic markers.
This hierarchy keeps longevity framing anchored to durable outcomes. A program can produce dramatic Tier 3 changes and still underperform on Tier 2 if function declines. High-quality programs protect all three tiers, with priority set by medical risk and long-horizon resilience. The hierarchical approach prevents short-sighted focus by ensuring that short-term metabolic improvements do not come at the expense of long-term functional capacity, thereby aligning treatment goals with genuine healthspan extension objectives.
Implementation Blueprint For 2026 Programs
Baseline
Collect strength and activity baseline, waist and composition proxy, blood pressure, glycemic markers, and symptom profile before dose escalation. Without baseline measurements, interpretation quality drops immediately. Include grip strength measurement, gait speed assessment, and basic mobility testing to establish functional benchmarks that will inform subsequent intervention adjustments and outcome evaluations.
First 90 days
Track adherence, appetite shifts, protein adequacy, and progressive resistance execution. Early warning signs include rapid weight loss with declining performance markers or persistent fatigue that reduces training tolerance. Implement weekly monitoring of strength training volume and intensity alongside dietary protein tracking to ensure lean mass preservation during the initial rapid weight loss phase that typically characterizes treatment initiation.
Quarterly governance
Review medication effect, function trend, body composition direction, and side-effect burden together. Adjust protocol if function and composition diverge from target state. Incorporate dual-energy X-ray absorptiometry (DXA) scans or bioelectrical impedance analysis at minimum to objectively quantify lean mass changes. Adjust exercise prescription and nutritional support based on quantitative data rather than subjective assessment alone.
Longevity Positioning: Bridge Technology, Not Final Architecture
GLP-1 class therapies can reduce near-term disease burden now and create a practical bridge while deeper interventions mature. That bridge remains valuable even if future reprogramming or senescence-targeting platforms prove superior in specific indications. The present objective is not ideological rigidity. It is measurable risk reduction with preserved function. These agents represent an intermediate therapeutic class that addresses multiple aging hallmarks simultaneously—particularly deregulated nutrient sensing and mitochondrial dysfunction—while more targeted gerotherapeutic approaches undergo development and validation.
The field now has enough data to act, and enough uncertainty to require disciplined execution. The convergence of robust clinical evidence with practical implementation challenges creates both opportunity and responsibility for clinicians to develop sophisticated treatment protocols that maximize benefit while minimizing treatment-related risk in pursuit of genuine healthspan extension.
Source List
Lincoff, A. M., et al. (2023). Semaglutide and cardiovascular outcomes in obesity without diabetes. New England Journal of Medicine.
Perkovic, V., et al. (2024). Semaglutide and renal outcomes in type 2 diabetes and CKD. New England Journal of Medicine.
Nature Biotechnology. (2025). When does anti-ageing become medicine?.
Tinsley, G. M., et al. (2025). Preservation of lean soft tissue during GLP-1 receptor agonist weight loss. Nutrients.
Hitaka, K., et al. (2026). Efficacy of GLP-1 analog peptides and tirzepatide in obesity treatment. International Journal of Obesity.