Digital Twins for Aging: Predictive Biology at Scale
The phrase digital twin attracts two opposite mistakes. One camp hears software marketing and dismisses it. The other hears full-body simulation and assumes medicine is close to a computable replica of each person. Aging research sits between those errors. The field is building stronger multimodal prediction systems that can represent trajectories of decline, resilience, and treatment response. It is not yet building a complete causal duplicate of a human organism that can be safely trusted as a substitute for longitudinal reality.
Established fact: biomedical prediction is improving as longitudinal clinical data, wearables, imaging, proteomics, and other omics become easier to integrate at cohort scale. Established fact: aging is especially suited to this style of modeling because it unfolds across years, leaves signal in multiple tissues, and is already tracked through clocks, functional tests, disease incidence, and survival. Established fact: the field still lacks a validated whole-person aging twin that can reliably predict intervention response across organs and timescales. The practical reading is narrower and more useful. Aging digital twins are becoming credible as layered forecasting systems. They are not yet mature as mechanistically complete substitutes for experiment.
Core thesis: digital twins for aging should be treated as predictive biology stacks, not as literal virtual humans. The near-term value is risk stratification, trajectory forecasting, and intervention ranking across richer data streams. The near-term limit is causal incompleteness. Scale is arriving faster than validated control.
What A Digital Twin Means In Aging Research
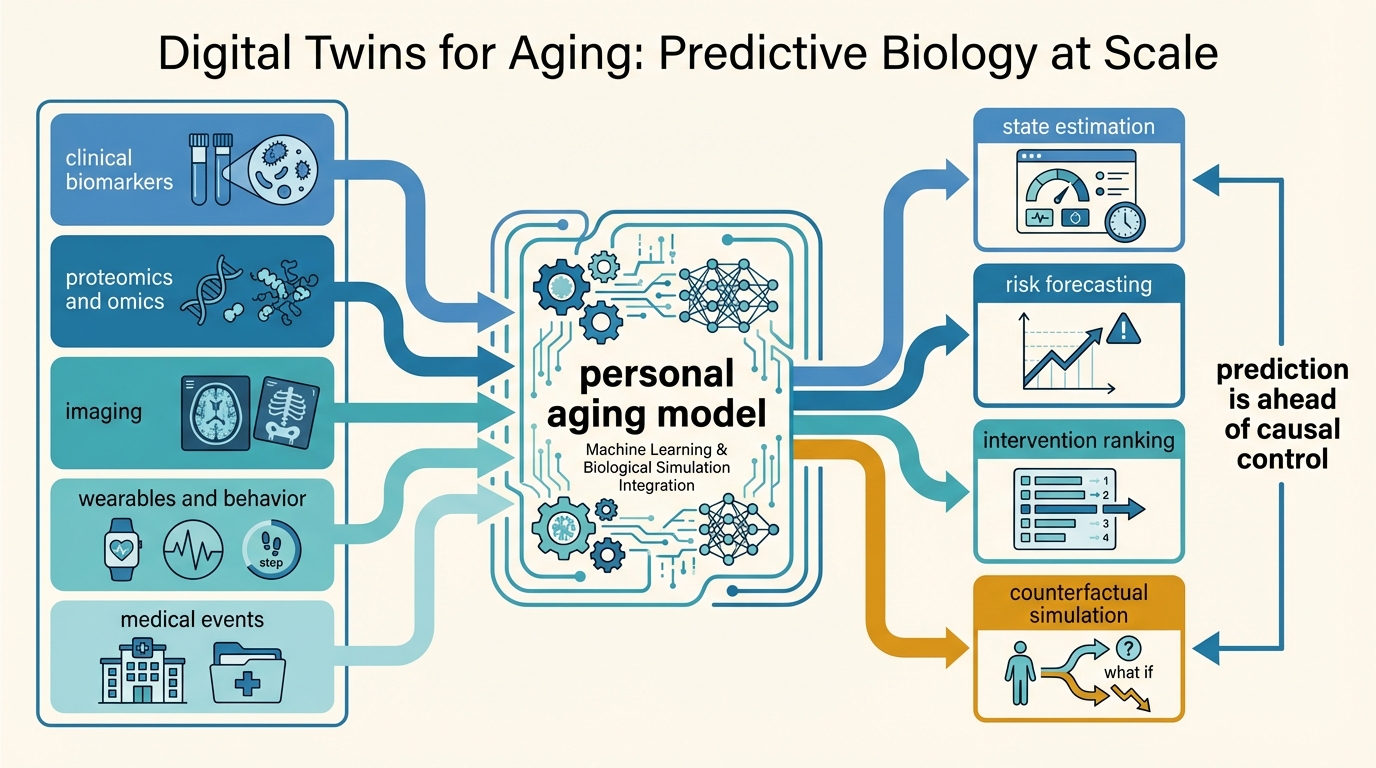
In engineering, a digital twin is a dynamic model linked to a real asset and continuously updated by incoming data. In medicine, that concept loosens because the system is vastly more complex and partly unobserved. For aging, the useful definition is a computational representation of an individual or cohort that updates from multimodal data and estimates future biological state under different conditions. That representation may include organ-specific clocks, risk scores, mechanistic submodels, treatment-response priors, and state-transition forecasts. It does not need to simulate every molecule to be useful. It does need to outperform simpler baselines on real clinical or functional tasks.
This distinction matters because aging is not one variable. It is a distributed process that includes cellular maintenance failure, chronic inflammation, tissue remodeling, metabolic change, immune drift, and cumulative disease burden. A serious digital twin therefore cannot rely on one clock score alone. It has to ingest multiple signals that move at different speeds and reflect different failure modes. That is why the most credible path is modular. One layer may predict cardiovascular aging from proteomics. Another may infer frailty or sleep disruption from wearables. Another may use imaging or retinal features. The twin is the integration logic across those modules.
The field already has pieces of this architecture. Organ-specific aging clocks can estimate differential aging burden across systems. Longitudinal patient-trajectory models can forecast short-horizon health states. Wearables can generate dense behavioral and physiological traces. Retinal, proteomic, epigenetic, and clinical-laboratory models can all contribute state information. The gap is not whether these components exist. The gap is whether they can be validated together in a way that supports intervention decisions instead of descriptive analytics alone.
Why Aging Is A Natural Use Case
Aging is unusually compatible with digital-twin logic because its main problem is trajectory management under uncertainty. Clinicians and individuals want to know who is aging faster than expected, which systems are diverging first, and whether a change in behavior, medication, or environment is likely to alter the path meaningfully. Static diagnostics are poor at that task. A longitudinal model is better suited because it can compare present state with expected future state and ask how strongly an intervention might move the curve.
This is one reason aging clocks became strategically important even when many early claims were overstated. A clock is not the twin. It is one instrument that helps define latent biological state. The same logic applies to continuous glucose data, sleep regularity, heart-rate variability, activity patterns, inflammatory proteins, or imaging markers. Each signal is partial. Together they offer a chance to estimate a more realistic future than any one biomarker can provide.
That said, aging also exposes the hardest weakness in the concept. Prediction across a natural history is easier than counterfactual prediction under intervention. A model may forecast that a person is on a faster path toward frailty or cardiometabolic disease. It is much harder to prove that the same model can tell which treatment will improve that path, by how much, over what time window, and with what tradeoffs across organs. This is the boundary between monitoring intelligence and intervention intelligence.
What The Best Current Evidence Actually Shows
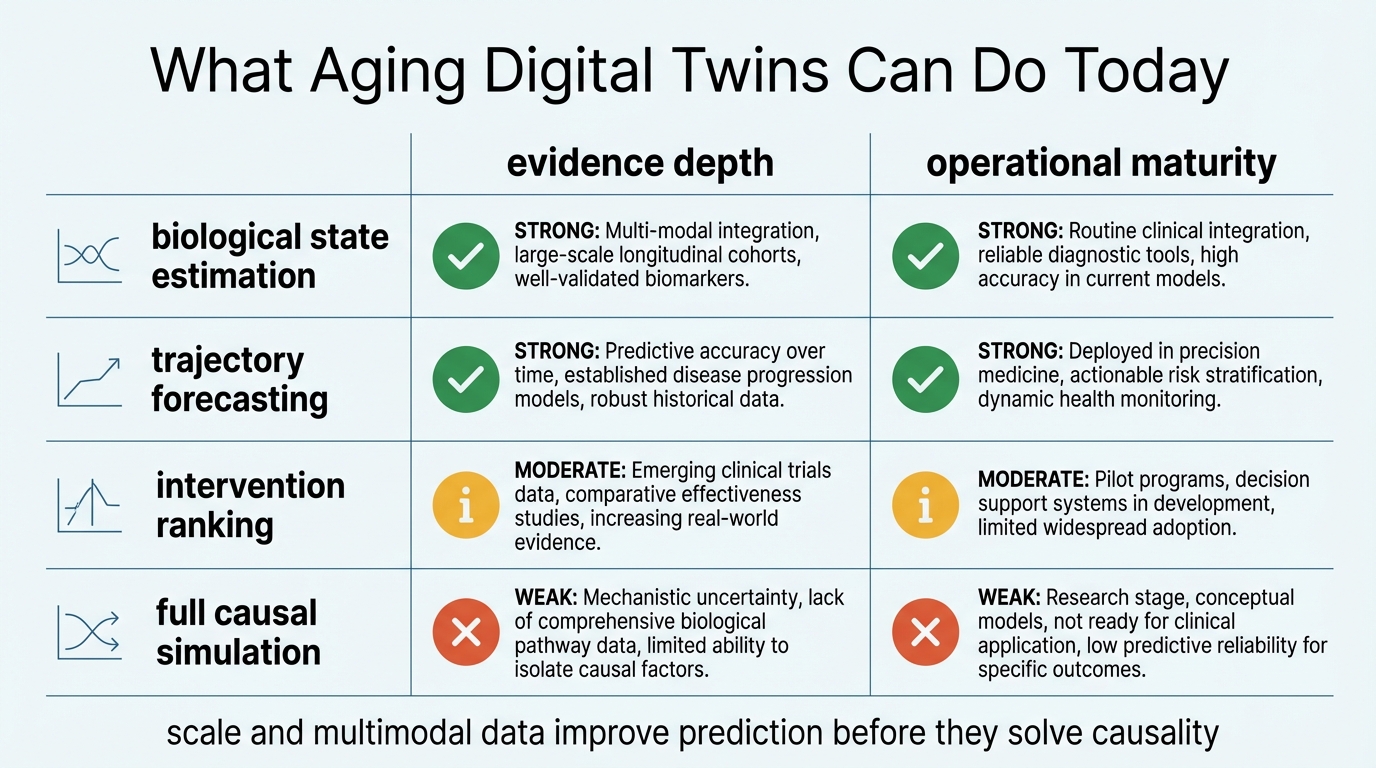
The strongest evidence today supports the claim that multimodal data can estimate aging state and disease risk better than sparse, single-channel measurement. Studies of organ-specific proteomic clocks show that biological aging does not proceed uniformly across systems and that organ age gaps carry predictive signal for mortality and disease. Retinal and other imaging-based models also show that accessible peripheral data can encode broader systemic aging information. Reviews of biomedical digital twins point in the same direction: the field is moving toward data-linked representations that can update, forecast, and personalize.
The strongest evidence does not yet support the more ambitious claim that a digital twin can serve as a robust substitute for human interventional trials in geroscience. Most models remain narrow in domain, cohort-specific in training, or dependent on surrogate endpoints. Even when performance is strong, the question is usually prediction over existing data structure, not validated control of future intervention response. That is why a good paper in this area often proves less than the headline suggests. It may establish that a model can compress large heterogeneous data into a useful state estimate. It does not automatically establish that the state estimate is causal enough to guide therapy selection safely.
This is where terminology can become misleading. The public hears twin and imagines full-person fidelity. The literature often uses the term more flexibly to describe a computational mirror whose fidelity is task-specific. For aging, that narrower meaning is defensible. A twin that predicts who is likely to deteriorate faster and flags which system should be monitored more closely may be clinically valuable even if it remains incomplete as a mechanistic simulator.
Where Predictive Biology At Scale Changes The Game
Scale matters because aging is heterogeneous. Small studies can show signal, but they often fail to capture the combinatorial diversity of medication use, ancestry, environment, fitness, disease burden, sleep pattern, socioeconomic stress, and baseline physiology that shape real aging. Large biobanks and healthcare datasets reduce some of that problem. Wearables reduce another part by adding longitudinal density rather than one-off snapshots. Together they allow models to move from cross-sectional association toward individual trajectory estimation.
That scale also creates a new practical possibility: intervention ranking. A model does not need to prove exact causal destiny to be useful. It may still rank plausible next moves better than unaided intuition. For example, a twin might identify that poor sleep regularity and rising inflammatory burden are contributing more to a person's projected decline than slight variation in one metabolic marker. Or it might show that cardiovascular and renal aging burden are separating from chronological age faster than other systems. Those are not magic answers. They are better triage.
The crucial caveat is transportability. A model trained on one cohort may fail when behavior patterns, measurement devices, disease prevalence, or treatment standards change. Aging digital twins therefore need repeated external validation and recalibration. This requirement is not bureaucratic. It is central to whether scale creates real utility or just bigger overfitting.
Where The Hype Usually Fails
The first failure is to treat prediction accuracy as proof of causal understanding. A model may forecast decline well because it captures dense correlations. That does not mean it knows which lever changes the future most effectively. Aging systems are full of coupled processes and hidden variables. Correlation-rich performance can still break when intervention shifts the system away from observed history.
The second failure is endpoint inflation. A digital twin that predicts a laboratory or clock outcome is not necessarily predicting function, disease-free survival, or resilience. This is the same caution LifeMeter applies to Biological Age Clocks as Decision Tools. A useful marker is not the same thing as a sufficient decision standard.
The third failure is interface theater. It is easy to wrap a dashboard around model outputs and imply comprehensive precision. The underlying question remains basic. Does the system improve real decisions relative to simpler clinical judgment, fewer biomarkers, or plain longitudinal follow-up? If not, sophistication in presentation is not sophistication in medicine.
What A Serious Aging Digital Twin Standard Would Require
- Task specificity. The model should state whether it is estimating biological state, forecasting risk, ranking interventions, or simulating treatment response. Those are different claims.
- Multimodal anchoring. Useful aging twins should combine at least some mix of clinical measures, longitudinal physiology, omics, imaging, or functional outcomes rather than relying on one proxy channel.
- External validation. Performance has to hold across cohorts, devices, and healthcare settings, not only in the training environment.
- Intervention testing. If a system claims actionability, it should be evaluated on whether its recommendations improve outcomes, not only on whether its forecasts look plausible.
- Human-readable uncertainty. Outputs should distinguish strong prediction, weak extrapolation, and unknown territory clearly enough for clinical use.
This standard is stricter than most marketing because the field is already good enough to tempt overclaiming. The better the models get, the more discipline is needed in how their outputs are interpreted.
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | Longitudinal multimodal data can capture meaningful aging-related state information across organs, physiology, and disease risk better than sparse one-time measurement. |
| Known | Current biomedical digital-twin work is strongest in prediction, monitoring, and risk stratification, not in complete causal simulation of an individual's future under intervention. |
| Known | Organ-specific and modality-specific aging models show that aging heterogeneity is measurable and clinically relevant, which supports modular twin architectures. |
| Inferred | The near-term practical value of aging digital twins will likely come from better triage and intervention ranking before it comes from precise treatment simulation. |
| Unknown | How much multimodal density and causal structure are necessary before an aging digital twin can reliably guide individualized intervention choices across diverse populations and long time horizons. |
The Practical Reading For 2026
For longevity analysis, the useful stance is neither dismissal nor surrender to hype. Digital twins for aging are real enough to matter because predictive biology is becoming richer, denser, and more personalized. They are not yet mature enough to be treated as definitive virtual patients. A strong model can help decide what to watch, what to test next, and which risk domains deserve attention. It still needs validation before it can justify confident intervention sequencing.
This is why the topic belongs alongside AI + Systems Biology for Biological Age Clocks, Biological Age Clocks as Decision Tools, and AI-Accelerated Drug Discovery in Aging. All three point to the same structural lesson. Computation is improving faster than endpoint certainty. The winners will be programs that respect that asymmetry rather than hide it.
Further Reading Inside The Site
This article connects directly to AI + Systems Biology for Biological Age Clocks, Biological Age Clocks as Decision Tools, and AI-Accelerated Drug Discovery in Aging. Together they frame how measurement systems, model architecture, and translational bottlenecks fit into one aging-intelligence stack.
Source List
Rasheed S, Qamar S, Zia MF, et al. Digital twins of biological systems: A systematic review. npj Digital Medicine. 2024.
Hajjar I, Xu C, Rueda G, et al. Digital twins for older patients: promises and challenges. npj Digital Medicine. 2025.
Bica I, et al. Generalized forecasting of patient trajectories with multimodal LLMs for digital twins in medicine. Nature Medicine. 2025.
Tian Y, et al. Multimodal retinal aging clock analysis identifies accelerated aging and risk factors. Nature Medicine. 2025.
Thareja G, et al. Organ-specific proteomic aging clocks predict disease and longevity across diverse populations. Nature Aging. 2025.
Frontiers in Aging. Wearable technologies and digital biomarkers in the context of aging and geriatrics. 2025.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.