Longevity Clinics: Science, Protocols, and Variability
Longevity clinics promise a cleaner future than ordinary medicine offers: more measurement, earlier intervention, and a direct operational response to aging before disease is obvious. The attraction is understandable. Standard care is often reactive, brief, and fragmented. The harder truth is that most longevity clinics are not practicing one mature clinical discipline. They are combining several evidence layers at once, and the quality of those layers differs sharply.
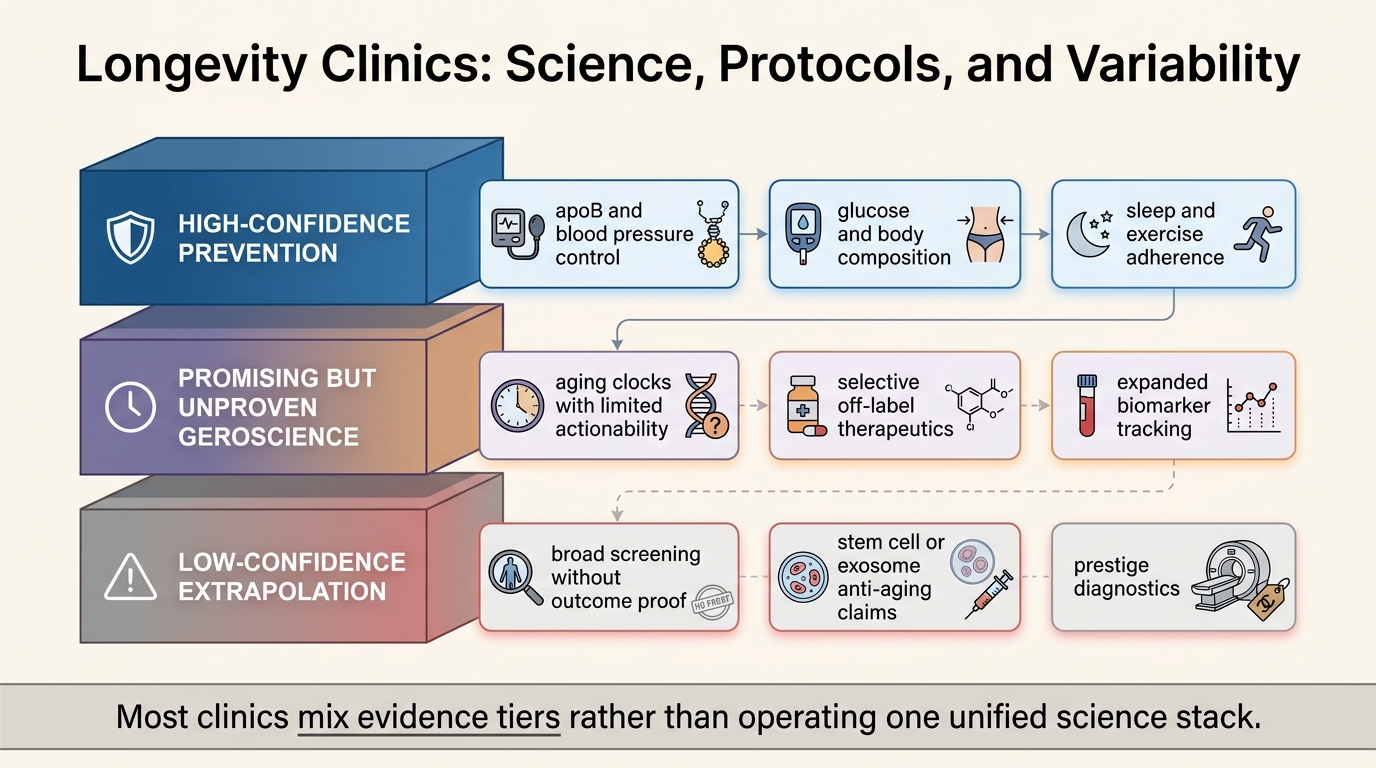
The most useful way to read the field is not to ask whether longevity clinics are real or fake. That framing is too crude. The better question is what parts of a clinic are grounded in established prevention, what parts are reasonable but still exploratory geroscience, and what parts are mostly commercial packaging around uncertainty. Once that separation is made, protocol variability stops looking mysterious. It starts looking like the predictable result of weak standardization, mixed evidence, and different business models solving different customer problems.
Core thesis: the strongest longevity clinics are usually delivering familiar medicine with more discipline: cardiometabolic risk reduction, body-composition management, sleep and exercise adherence, and tighter longitudinal follow-up. The weakest clinics blur that high-confidence layer with aging clocks treated as control panels, broad screening with uncertain net benefit, and anti-aging therapeutic claims that remain under-validated in humans. Protocol variability is mostly a signal that the evidence stack is still uneven.
What The Best Clinics Are Actually Doing Well
The best clinics are usually not performing miracles in aging biology. They are reducing ordinary clinical drift. They identify elevated apoB earlier, treat blood pressure more aggressively, track glucose and body-composition change over time, push cardiorespiratory fitness and resistance training harder, and create a follow-up cadence that conventional reimbursement often does not support. None of that is trivial. It can improve health materially. It also does not require exaggerated anti-aging language to justify itself.
This matters because the highest-confidence part of longevity medicine is still risk-factor medicine. Common clinical biomarkers already predict disease-free survival and lifespan directionally. That does not mean every biomarker extension is useful, but it does mean a clinic can create real value simply by measuring important variables consistently and acting on them earlier. The durable medical logic is usually strongest where the intervention pathway is already well understood.
That is why some clinic outcomes feel impressive even when the underlying science is ordinary. Better adherence, more time per patient, tighter monitoring, and faster treatment escalation can look futuristic because routine care often undersupplies them. Readers should not confuse that delivery advantage with proof that the clinic has solved human aging as a clinical endpoint problem.
Where The Evidence Starts To Thin Out
The weaker zone begins when clinics imply that more measurement automatically produces more useful action. That inference often fails. A marker can be analytically interesting without being ready for confident clinical steering. Aging clocks are the clearest example. Research in this area is expanding quickly, and some clock designs correlate with risk better than older broad estimates. Even so, the field still faces unresolved questions about what a given clock is measuring, how stable the estimate is across platforms and tissues, how much decision uncertainty should be attached to any single reading, and whether clock movement from an intervention reliably predicts durable human benefit.
That gap matters because clinics often sell clocks as if they were navigation instruments rather than research-adjacent summaries. A biological age estimate can be suggestive and still fail the harder clinical question: what exact decision changes because of this number, and what evidence says that change improves long-horizon outcomes beyond established risk assessment? When that question has no clear answer, the clinic is operating more like an innovation showroom than a settled care pathway.
The same caution applies to broad testing packages. Expanded blood panels can be reasonable when the additional markers feed a defined decision process. They become weaker when they are used to manufacture the feeling of precision without a corresponding treatment hierarchy. A serious protocol should explain why each measurement exists, what threshold or trajectory matters, and what action follows. Many clinic menus do not provide that clarity.
Why Screening Can Be Both Attractive And Misleading
Whole-body imaging and high-density screening are especially easy to oversell because they match the consumer fantasy of finding hidden problems before symptoms appear. The complication is that detection is not the same thing as net benefit. The literature on preventive whole-body MRI has long emphasized incidental findings, follow-up cascades, false reassurance in some domains, anxiety in others, and uncertain outcome improvement when asymptomatic people are screened broadly. A clinic that markets more imaging as straightforward prudence is compressing a much more complicated evidence story.
This does not mean that all aggressive screening is wrong. It means screening quality depends on population selection, downstream management, and the discipline to distinguish meaningful signal from noise. The business pressure inside membership medicine runs in the opposite direction. More diagnostics are easy to display and easy to bill for. The burden of proving clinical value is harder. That asymmetry is one major reason protocols diverge.
Readers should therefore ask a narrow question whenever a clinic recommends a broad panel or imaging layer: what bad outcome is this supposed to prevent, in what risk group, and what will we do differently if the result is positive, equivocal, or incidental? If the answer is vague, the diagnostic sophistication may be more aesthetic than medical.
Why Therapeutic Stacks Diverge Even More Than Diagnostics
Therapeutics create the widest variation because the evidence tiers widen sharply once clinics move beyond established prevention. Some stay close to mainstream practice: lipid-lowering, blood-pressure control, obesity treatment, sleep-disorder management, and structured exercise support. Others add off-label drugs, peptides, hormone optimization, stem-cell-adjacent claims, or exosome and regenerative language. At that point the clinic is no longer only packaging better prevention. It is choosing how far to front-run incomplete geroscience.
Human anti-aging evidence remains much thinner than clinic branding often suggests. That is especially clear where FDA has repeatedly warned consumers about unapproved regenerative medicine products, including stem cells and exosomes, and has continued enforcement against firms making anti-aging or broad treatment claims without approval. A clinic that presents these interventions as mature longevity medicine is stepping well outside the strongest evidence zone.
Even the more respectable edge of the field still faces endpoint problems. A mechanistically plausible intervention can produce biomarker movement, inflammation changes, or favorable animal data without yet proving broad human healthspan benefit. That does not make the intervention useless. It means the clinic should label the uncertainty plainly. The critical failure is not experimentation itself. The critical failure is pretending that exploratory translation already counts as validated clinical practice.
Why Protocol Variability Is Structurally Hard To Eliminate
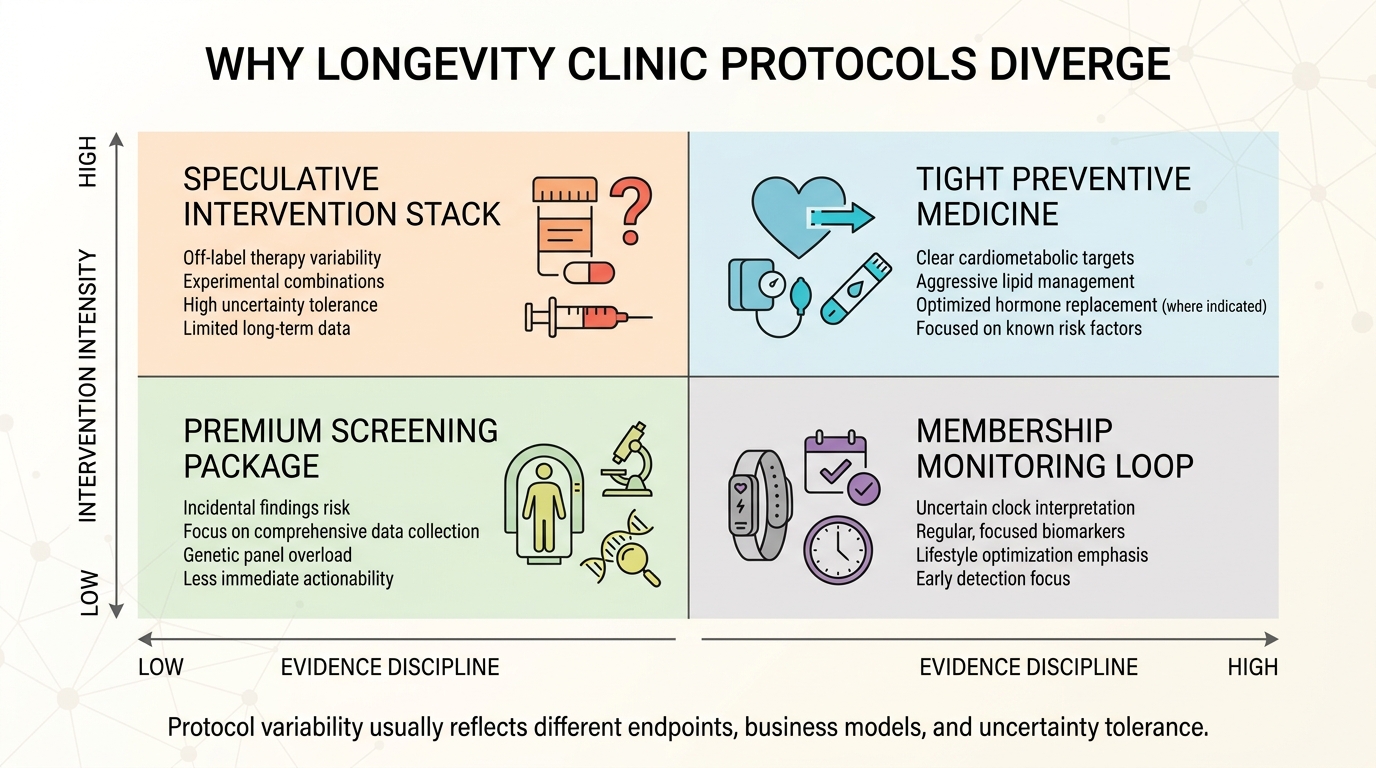
Conventional medicine converges because reimbursement, specialty training, guidelines, and liability pressure push clinicians toward narrower standard pathways. Longevity clinics operate under looser conditions. They compete on time, personalization, prestige, and novelty. That environment rewards experimentation and package differentiation more than it rewards standardization around long-horizon evidence. Variability is therefore not an accident. It is a structural feature of the market.
There is also an endpoint problem at the center of the field. Clinics are not all optimizing for the same thing. Some want lower cardiovascular risk. Some want better visible aging markers, body composition, or performance. Some want recurring member engagement through dense monitoring. Some want to position themselves at the frontier of geroscience. Different endpoints produce different protocols, even before one asks whether the endpoint itself is valid.
This is why serious readers should stop treating the phrase longevity clinic as if it identified a coherent category. It does not. It labels a spectrum that ranges from premium preventive medicine to speculative intervention retail. The same storefront can contain both at once.
What A High-Integrity Clinic Would Make Explicit
- It would tier the evidence. Established prevention, plausible but unproven translation, and low-confidence speculation would be labeled separately.
- It would tie every marker to a decision rule. Measurement would not be justified by novelty alone.
- It would explain downside, not only upside. Incidental findings, overtreatment risk, and uncertainty in interpretation would be part of the consent logic.
- It would avoid using anti-aging language to upgrade ordinary care into claimed age reversal. Better prevention is valuable on its own terms.
- It would prefer functional outcomes to dashboard theater. Strength, aerobic capacity, metabolic control, sleep, and symptom burden matter more than decorative data density.
The interesting result is that the highest-quality clinic might look less radical than the most heavily marketed one. It would probably be more conservative in claims, more explicit about uncertainty, and more selective about intervention creep. That can feel less exciting to consumers who are paying for frontier access. It is still closer to what the evidence currently supports.
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | Cardiometabolic and other common clinical biomarkers can help predict healthspan and lifespan risk, which supports the strongest preventive layer inside clinic practice. |
| Known | Aging clocks remain scientifically active but still face unresolved clinical-implementation questions around meaning, uncertainty, and actionability. |
| Known | Broad preventive screening can generate incidental findings and uncertain net benefit when used aggressively in asymptomatic populations. |
| Known | FDA continues to warn against unapproved regenerative medicine and anti-aging product claims, especially around stem cells and exosomes. |
| Inferred | Much of the real value some longevity clinics provide today comes from better preventive execution rather than from validated age-modifying therapeutics. |
| Unknown | Which clinic protocol bundles will still look superior once tested against long-horizon human outcomes rather than short-interval biomarker movement and member satisfaction. |
The Practical Reading For 2026
Longevity clinics are most defensible when they operate as disciplined translators between underused preventive medicine and carefully bounded experimentation. They become weak when they compress every interesting signal into the language of clinical certainty. Readers should therefore audit the protocol layer by layer. What is ordinary but valuable. What is plausible but still exploratory. What is essentially prestige medicine wrapped in geroscience vocabulary.
That discipline matters because the field will probably mature unevenly. Some currently speculative tools may become genuinely actionable. Others may remain attractive abstractions that perform better in marketing than in medicine. The safest present-tense conclusion is narrower: longevity clinics can be useful, but their usefulness depends less on how futuristic they look than on how honestly they separate established care from inference.
Further Reading Inside The Site
This article connects directly to Is Aging a Disease or an Adaptive Program?, Biological Age Clocks as Decision Tools, and AI-Designed Longevity Drugs: Early Successes and Limits. Together they show why translational excitement, endpoint discipline, and clinical reality have to be kept separate.
Source List
Li X, Ploner A, Wang Y, et al. Clinical Biomarkers and Associations With Healthspan and Lifespan: Evidence From Observational and Genetic Data. EBioMedicine. 2021.
Fong S, Pabis K, Latumalea D, et al. Principal Component-Based Clinical Aging Clocks Identify Signatures of Healthy Aging and Targets for Clinical Intervention. Nature Aging. 2024.
Kriukov D, Efimov E, Gelfand MS, et al. Do We Actually Need Aging Clocks?. npj Aging. 2026.
Kwee TC, Kwee RM. Whole-Body MRI for Preventive Health Screening: A Systematic Review of the Literature. Journal of Magnetic Resonance Imaging. 2019.
U.S. Food and Drug Administration. Consumer Alert on Regenerative Medicine Products Including Stem Cells and Exosomes. Updated July 22, 2020.
U.S. Food and Drug Administration. Dynamic Stem Cell Therapy Warning Letter. February 11, 2026.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.