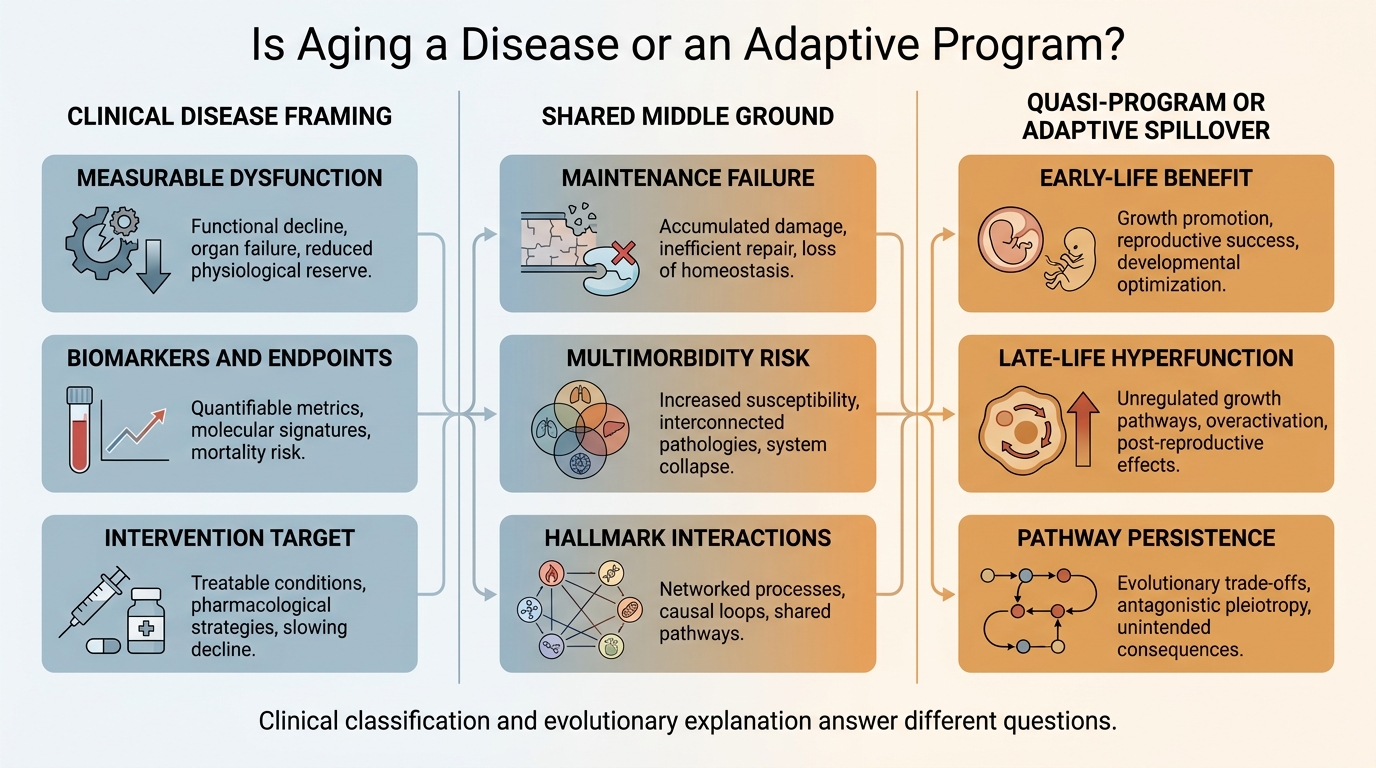
Is Aging a Disease or an Adaptive Program?
The debate stays confused because one phrase is doing three jobs at once. The disease framing asks how medicine should classify and treat aging. The adaptive-program or quasi-program framing asks why some late-life decline looks organized rather than purely accidental. The strongest 2026 position is layered: aging behaves like a disease-generating process clinically, while mechanistically it mixes damage, repair failure, and the late-life continuation of pathways that were useful earlier in life.
The distinction matters because clinical translation and evolutionary explanation are not the same problem. If aging is treated as a disease target, it becomes easier to justify biomarkers, endpoints, reimbursement logic, and development programs aimed at upstream mechanisms rather than only downstream pathologies. If aging is discussed as a program, the real question is narrower: did evolution select late-life decline itself, or do some harmful late-life states arise because growth, fertility, repair, and nutrient-sensing systems continue operating outside the window where they were beneficial? A single slogan hides those differences.
Core thesis: treating aging as a disease is increasingly useful for translational medicine because it is measurable, modifiable in model organisms, and upstream of multiple pathologies. Calling aging an adaptive program is too strong if it implies a single organism-level death script. The more defensible claim is narrower: some components of aging behave like quasi-programs or late-life spillovers of pathways that improved early-life fitness. The strongest synthesis is pragmatic disease framing plus mixed-mechanism biology.
Why The Disease Framing Keeps Gaining Ground
The case for disease classification starts from intervention logic. Aging is tightly linked to multimorbidity, frailty, and mortality risk. It produces measurable changes across hallmarks, biomarker systems, and functional decline. In model organisms, altering nutrient sensing, senescence burden, mitochondrial quality control, autophagy, and stress-response pathways can extend lifespan or health span. That makes aging different from a vague philosophical condition. It behaves like a modifiable causal substrate.
This is why the disease argument keeps resurfacing in policy and geroscience. Once aging is treated as a legitimate target, the field can justify trial design around upstream mechanisms rather than waiting for one disease at a time to appear. Zhavoronkov and Bhullar made this point directly in the ICD-11 discussion: the absence of a clean disease label for aging creates a translational bottleneck because reimbursement, endpoint validation, and regulatory design become harder when the core process is left unnamed.
The hallmarks framework strengthened that case. The 2013 Cell paper and the 2023 expansion did not define aging as a disease in regulatory language, but they did something close at the mechanistic level. They presented aging as a tractable bundle of interacting lesions and maintenance failures. Once those layers can be measured and perturbed, the distinction between aging and treatable causal process becomes less rigid than older medical language implies.
That does not mean aging is identical to pneumonia or leukemia. Disease categories in medicine are partly pragmatic. They are tools for describing dysfunction, risk, and intervention pathways. On that pragmatic standard, aging increasingly behaves like a disease process or, more precisely, a disease-generating process. The point is not that aging must be morally pathologized. The point is that medicine needs a usable framework for targeting it.
Why Quasi-Program Thinking Still Matters
The strongest version of the adaptive-program claim is not that evolution wanted old organisms to decline for their own sake. That version remains weak because natural selection is strongest earlier in life, when reproduction and survival materially affect fitness. The more serious claim is that late-life decline can emerge from pathways that were selected for growth, fertility, repair, or competitive performance earlier on. In that view, aging can reflect persistence, overactivity, or dysregulation of once-beneficial programs in a period when selection pressure has already faded.
This is where antagonistic pleiotropy and quasi-program theories matter. Antagonistic pleiotropy proposes that genes can be favored because they improve early-life fitness even if they impose later-life costs. Quasi-program theories go further by arguing that some age-related pathology is driven not mainly by random damage but by developmental or growth programs that continue beyond their useful domain. Blagosklonny's mTOR-centered quasi-program framing remains one of the clearest examples. The claim is not that aging is a neatly designed death program. The claim is that hyperfunctional continuation of growth-related signaling can generate age-related pathology.
That framing helps explain why some late-life biology looks organized rather than merely broken. Cellular senescence, chronic inflammation, fibrosis, and hypertrophic signaling often reflect pathways with real physiological roles in wound healing, development, immunity, or nutrient response. The problem is not that these systems are inherently pathological. The problem is that they can become persistent, miscalibrated, or insufficiently terminated in later life.
Seen this way, quasi-program thinking retains value because it prevents an overly simple wear-and-tear story. Organisms do not age only because molecules randomly erode. They also age because regulation, repair allocation, and growth-control systems can become maladaptive over time.
Where The Program Label Overreaches
Still, the phrase adaptive program often reaches too far. Adaptive for whom, and at what life stage, is the decisive question. There is limited evidence that late-life degeneration itself was broadly selected because it helps the organism. Most evolutionary frameworks still explain aging through declining force of selection with age, tradeoffs, imperfect maintenance, mutation accumulation, and early-life benefit versus late-life cost. That is not the same as a deliberate organism-level aging program.
This distinction matters because the adaptive label can mislead readers into thinking that aging is centrally orchestrated by a single master switch. The evidence does not support that. Some changes are stochastic and damage-linked. Some are failures of maintenance capacity. Some are downstream consequences of dysregulated pathways that remain active too long or respond too strongly. Any theory that compresses all of that into one mechanism loses explanatory power.
The 2023 hallmarks expansion reinforces the point. By separating chronic inflammation, disabled macroautophagy, and dysbiosis more clearly, the field became less compatible with single-cause storytelling. Aging now reads even more like a network with feedback loops than like a linear script.
A Better Synthesis
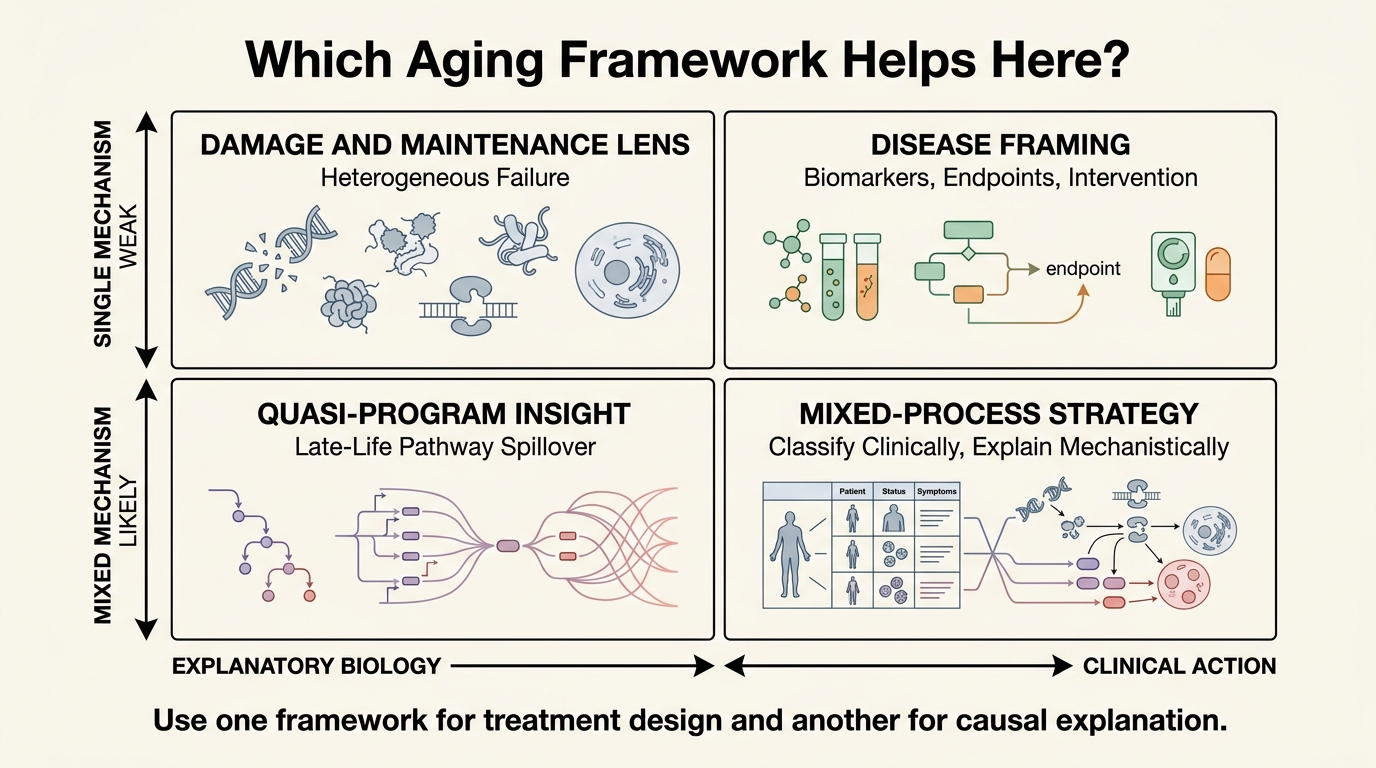
The strongest synthesis is layered. At the evolutionary level, aging is best explained by imperfect maintenance, declining force of selection with age, tradeoffs, and late-life spillover of pathways that were beneficial earlier. At the mechanistic level, aging is a network of interacting defects and maladaptive responses. At the clinical level, aging behaves like a disease-generating process that should increasingly be measured and targeted directly.
This layered view resolves several false choices. It allows medicine to classify aging in a way that supports intervention without claiming that all aging is one discrete disease entity. It also preserves the insight that late-life pathology sometimes comes from persistent biological programs, but without pretending that evolution designed a neat self-destruction module for old age.
In practical terms, this is why rapamycin, senolytics, exercise, dietary interventions, and regenerative strategies can all make sense inside one map. They do not all target the same thing. Some reduce damage or stress exposure. Some recalibrate nutrient sensing or inflammatory tone. Some clear harmful cellular states. Some restore maintenance capacity. A mixed-process theory makes room for that diversity. A single-cause theory struggles to do so.
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | The disease-classification camp argues that aging is measurable, causally upstream of many pathologies, and increasingly tractable for intervention, which makes a stronger clinical label useful. |
| Known | Evolutionary theories such as antagonistic pleiotropy and disposable-soma logic support the idea that late-life decline can result from tradeoffs and insufficient investment in long-term maintenance. |
| Known | Quasi-program theories propose that some age-related pathology reflects continued or excessive action of pathways that were beneficial earlier in life, especially growth-related signaling. |
| Inferred | The most useful current synthesis is mixed: aging includes damage accumulation, maintenance failure, and maladaptive continuation of earlier-life programs. |
| Unknown | How much of human aging burden is dominated by stochastic damage versus quasi-program behavior, and which intervention mix will matter most clinically across tissues. |
What This Means For Real Longevity Work
For translational longevity, the disease framing should probably win operationally. Drug development, biomarker qualification, reimbursement, and clinical adoption all work better when aging can be treated as a legitimate intervention target. The field does not need a perfect philosophical category before acting on a clearly harmful, measurable process.
For theory, adaptive-program language should be used more carefully. It is helpful when it points to late-life hyperfunction, antagonistic pleiotropy, and pathway persistence. It becomes unhelpful when it implies that aging is centrally intentional or uniformly programmed.
For readers trying to interpret longevity claims, the practical rule is simple. Ask whether a claim is about clinical classification, evolutionary cause, or intervention mechanism. Many apparent disagreements collapse once those levels are separated. Aging is a disease can be a clinically rational statement. Some aging processes look quasi-programmed can also be mechanistically rational. Confusion starts when either is mistaken for a complete theory of everything.
Further Reading Inside The Site
This article connects directly to Hallmarks of Aging Revisited: What Changed Since 2013, Senolytics Moving into Clinical Translation, and Stem Cell Exhaustion and Replenishment Strategies. Together they show why aging is more usefully handled as an intervention network than as a single slogan.
Source List
López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. The Hallmarks of Aging. Cell. 2013.
López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. Hallmarks of Aging: An Expanding Universe. Cell. 2023.
Zhavoronkov A, Bhullar B. Classifying Aging as a Disease in the Context of ICD-11. Frontiers in Genetics. 2015.
Blagosklonny MV. Rapamycin and Quasi-Programmed Aging: Four Years Later. Cell Cycle. 2010.
Kirkwood TBL. The Disposable Soma Theory of Aging. Progress in Brain Research. 1990.
Long H, Zhang Y, Zhang Y, et al. Evidence for the Role of Selection for Reproductively Advantageous Alleles in Human Aging. Science Advances. 2023.
World Health Organization. Ageing and Health. Updated October 1, 2024.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.