AI + Systems Biology for Biological Age Clocks
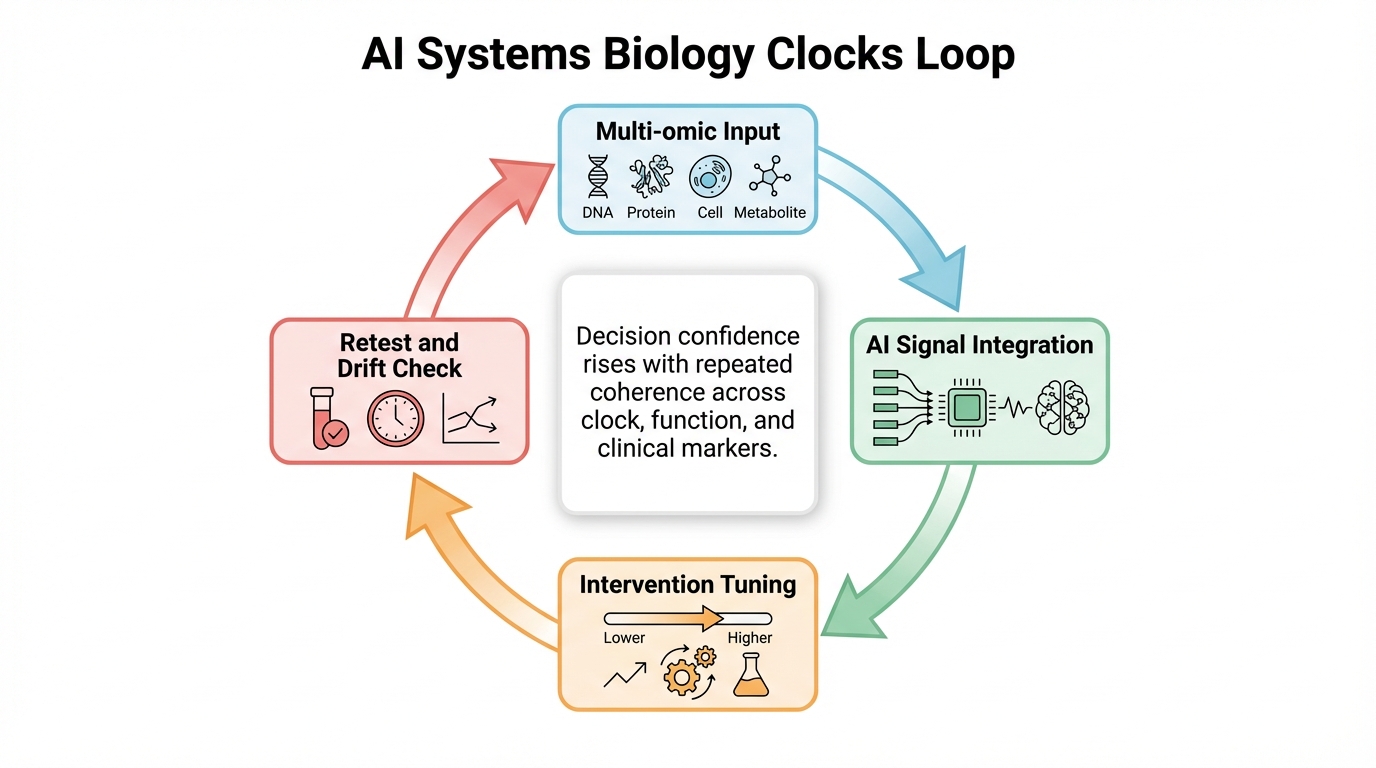
Aging clocks become clinically useful when AI integrates multi-omic and functional data in a repeatable loop. Without that loop, clock scores remain fragile signals prone to overinterpretation.
Biological age measurement is shifting from niche geroscience to practical decision support. This shift is driven by richer molecular profiling and better machine-learning integration across diverse signals. The opportunity is clear: reliable measurement of aging pace and intervention response materially improves treatment design. The constraint is equally clear: reliability, interpretability, and endpoint relevance still limit personal-level claims. Current systems biology treats aging as multidimensional, requiring multimodal assessment rather than single-metric reliance.
What Is Established
Clock science is robust at population scale
DNA methylation clocks and pace-of-aging models show reproducible associations with morbidity and mortality risk at the cohort level. This supports their use in risk stratification and longitudinal population science. These validations confirm biological aging metrics capture meaningful variance in healthspan outcomes across diverse populations. Large sample sizes enable detection of subtle associations invisible at individual levels.
Some interventions can shift pace metrics
In CALERIE, long-term caloric restriction shifted DunedinPACE toward slower biological aging. This does not prove universal reversibility, but shows pace metrics are modifiable in randomized human settings. Subsequent studies on exercise, pharmacology, and diet show varying degrees of clock modulation, suggesting distinct biological pathways influence measurements.
AI integration improves multi-signal interpretation potential
AI models integrate methylation, proteomic, metabolomic, and clinical time-series inputs into unified frameworks. In principle, this improves responsiveness and personalization over single-assay interpretation. In practice, model drift and cohort specificity require strict validation. Ensemble methods and transfer learning show promise for maintaining accuracy across physiological contexts.
What Remains Constrained
Single-person reliability and reproducibility
Assay and preprocessing variability can produce false movement at the individual level. Reliability methods exist, but operational quality depends on stable pipelines and repeat testing. Variables like collection timing, handling, and storage introduce noise that can obscure genuine signals. Protocols must account for diurnal variations, diet, and exercise effects that influence molecular readouts.
Interpretability for clinical decisions
A clock shift does not reveal causal mechanisms. The same numerical shift can arise from different processes. Without paired functional markers, interventions based on clock values alone can be miscalibrated. Translation requires knowing if clock changes reflect underlying aging hallmarks or statistical adjustments without physiological relevance. This determines whether clock-guided interventions yield meaningful health benefits.
Risk of optimization to the score
High-visibility metrics invite score-chasing. Clinical strategy should prioritize real outcomes, treating clock trajectories as one input. Manipulating readings via transient interventions poses a significant challenge. Sustainable protocols prioritize interventions with demonstrated healthspan benefits over isolated metric improvements.
Operational Framework For Clinical Use
Step 1: lock the measurement contract
Keep assay provider, sampling, pipeline, and model stable across repeated tests. Pipeline shifts reduce comparability and trend confidence. Establish baselines under standardized conditions before interventions, documenting all procedural variables. This consistency forms the foundation for meaningful longitudinal assessment.
Step 2: anchor to high-value outcomes
Track strength, aerobic capacity, blood pressure, glycemic control, body composition, and disease markers alongside clock data. These anchors reduce interpretive error. Functional assessments like cognitive performance and vascular health provide complementary validation. Convergence of molecular clocks with functional measures creates a robust framework.
Step 3: use interval discipline
Favor months over weeks for interpretation. Short windows capture noise or transient physiology rather than true trajectory changes. Establish minimum meaningful change thresholds based on variability and plausibility. Quarterly assessments offer better signal-to-noise ratios than frequent measurements while allowing timely adjustments.
Step 4: apply confidence tiers
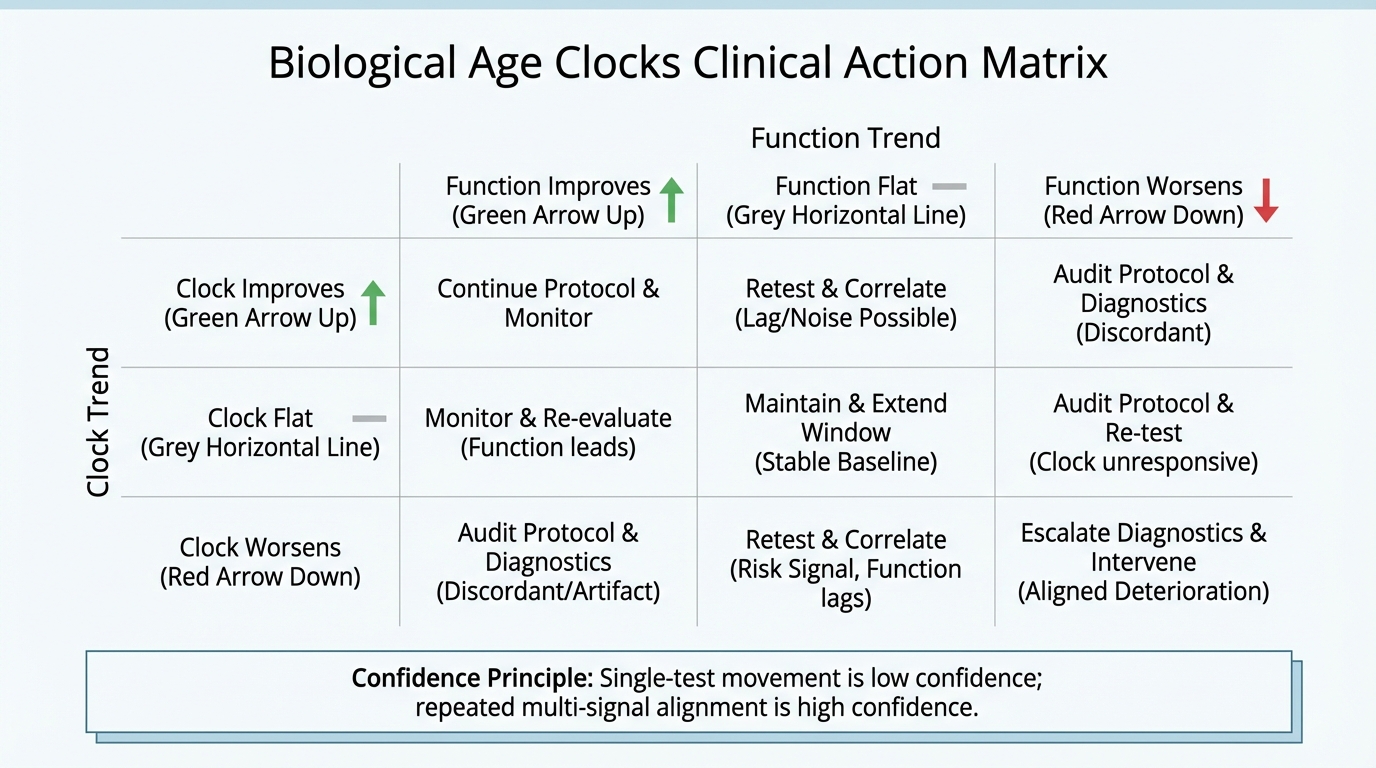
Highest confidence comes from repeated concordance between clock and clinical improvements. Medium confidence comes from clock-only directional consistency under stable conditions. Lowest confidence comes from isolated short-interval changes without endpoint support. Weight evidence by confidence level; higher tiers trigger significant intervention modifications.
Known: Clocks are useful for risk and trend analysis at the appropriate evidence layer.
Inferred: Multi-omic AI integration can improve personalization and response detection.
Unknown: How quickly clock-guided personalization translates into large-scale hard-outcome gains.
LEV Context: Why Measurement Infrastructure Matters
Longevity escape velocity narratives often emphasize intervention breakthroughs. Measurement quality is the other half. If interventions improve but feedback systems remain noisy, compounding slows as learning loops degrade. Reliable aging metrics are not an accessory to LEV; they are enabling infrastructure. Intervention targeting precision depends on measurement resolution, creating a symbiotic relationship between therapy and assessment.
Public forecasts remain broad. Kurzweil discusses late-2020s to mid-2030s windows. Others, including Aubrey de Grey, see material probability for 2030s scenarios. Timelines remain contingent on two bottlenecks: clinical validation and measurement reliability. AI aids both, but neither bottleneck is solved. Translating basic research into actionable protocols requires bridging population associations and individual predictions with sufficient accuracy.
Source List
Horvath, S. (2013). DNA methylation age of human tissues and cell types. Genome Biology.
Belsky, D. W., et al. (2022). DunedinPACE, a DNA methylation biomarker of pace of aging. eLife.
Waziry, R., et al. (2023). Caloric restriction and DNA methylation measures of biological aging (CALERIE). Nature Aging.
Higgins-Chen, A. T., et al. (2022). Bolstering reliability of epigenetic clocks for longitudinal tracking. Nature Aging.
Apsley, A. T., et al. (2025). Limits of epigenetic clocks as personal biomarkers in clinical translation. Geroscience.
Lieberwirth, J.-K., et al. (2026). Challenges and potential of digital biomarkers in clinical practice. Communications Medicine.