Caloric Restriction Mimetics: What Actually Works in Humans
The phrase "caloric restriction mimetic" still does too much rhetorical work. It groups together compounds that touch one nutrient-sensing pathway, compounds that improve a narrow clinical endpoint, and compounds that only look impressive in rodents. Those are three different evidentiary categories. Treating them as one category is how mechanism gets mistaken for translation.
The cleanest starting point is still the benchmark itself. The strongest human evidence belongs to calorie restriction, not to a capsule marketed as if it captured calorie restriction by analogy. CALERIE and related follow-up work showed that sustained energy restriction can move cardiometabolic risk, liver-related biomarkers, and parts of the senescence-associated secretome in controlled human settings. That does not prove lifespan extension. It does establish that the benchmark is broad, systemic, and difficult to mimic.
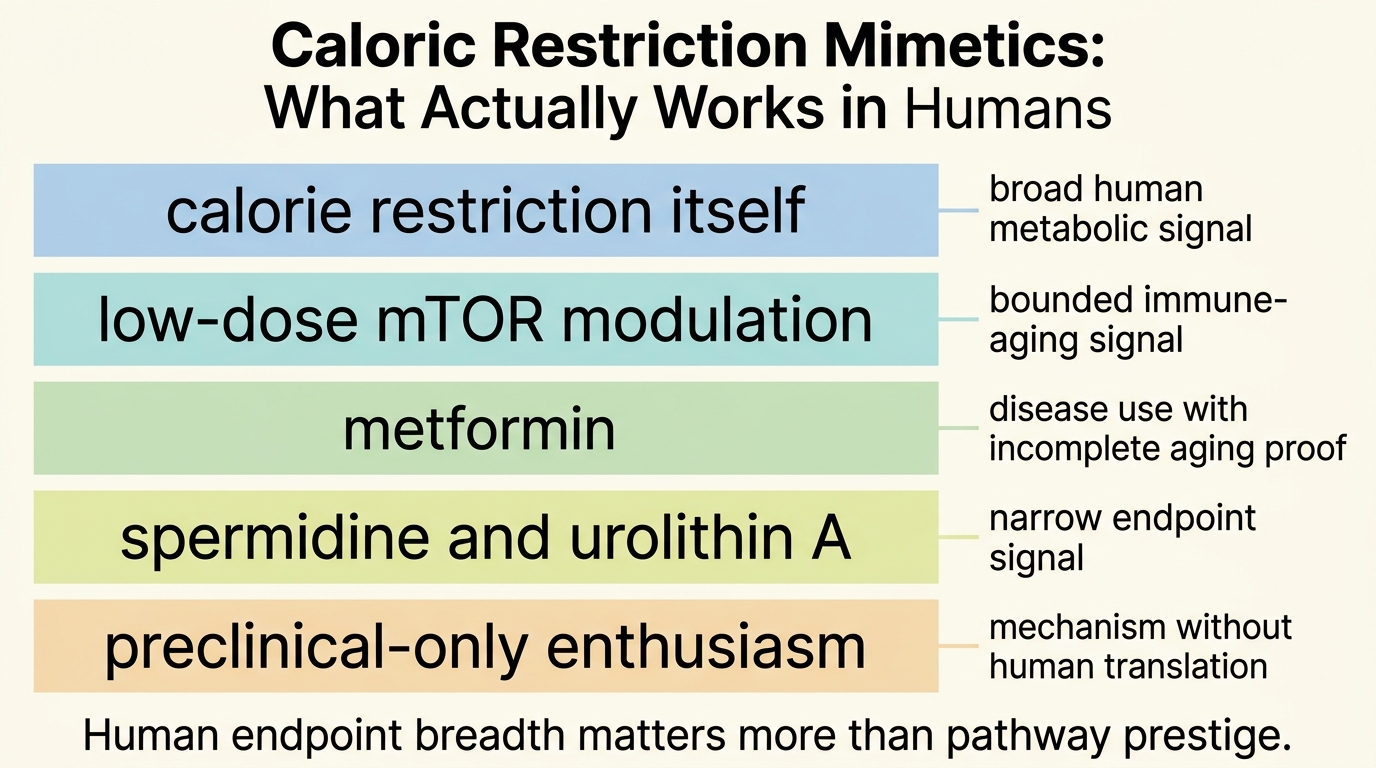
Core thesis: in humans, no compound has yet earned the status of a true caloric-restriction substitute. What exists instead is tiered evidence: calorie restriction itself has the clearest human signal; rapalogs, metformin, spermidine, urolithin A, and related candidates show narrower, endpoint-specific effects; lifespan extension in healthy humans remains unproven.
The Benchmark Is Calorie Restriction, Not Marketing Language
Real calorie restriction is inconvenient, adherence-limited, and biologically broad. That last point matters. Energy restriction does not move one marker. It changes insulin signaling, nutrient sensing, adipose biology, immune tone, body composition, and probably tissue repair dynamics across interacting systems. Mimetic claims usually enter by capturing only part of that network.
The 2-year CALERIE phase 2 trial matters because it gives the field a human reference case instead of a rodent slogan. The intervention lowered cardiometabolic risk burden, and later analyses reported movement in liver biomarkers and secretome-linked aging signals. That still falls short of direct lifespan proof. The relevant point is narrower and stronger: humans can show multi-system physiologic movement under sustained energy restriction. Any proposed mimetic should therefore be judged against breadth, persistence, and tradeoffs, not against a single pathway diagram.
Metformin: The Most Discussed Candidate, Still Not a Human Longevity Drug
Metformin remains the most discussed candidate because it is cheap, familiar, and biologically plausible. It improves glycemic control, alters hepatic glucose output, and touches AMPK-linked signaling. Epidemiology in people with type 2 diabetes has often suggested better-than-expected outcomes relative to comparison groups. That is relevant. It is still not the same as a randomized human aging result in broadly healthy adults, and it does not by itself justify treating metformin as a validated longevity drug.
The honest read remains narrower. Metformin clearly works as a diabetes drug. It may also improve selected aging-relevant processes in specific metabolic contexts. What it has not produced is a decisive human trial result showing broad aging-delay benefit outside disease treatment. The field still leans on the proposed TAME framework precisely because the definitive trial has not happened. That absence is informative. After years of attention, the strongest metformin claim is still disease management plus plausible geroscience relevance, not validated longevity translation.
Rapalogs: The Best Mechanistic Story, But Human Use Is Still Domain-Specific
mTOR inhibition has stronger aging credentials in animal models than most competitors, and rapamycin remains one of the few interventions that repeatedly extended lifespan across species. In humans, the translational question is not whether mTOR matters. It does. The question is whether controlled inhibition can produce enough benefit outside transplant or oncology settings without paying an unacceptable immune, metabolic, or tolerability cost.
The human data are promising but still specific. Trials with low-dose mTOR-pathway inhibition in older adults showed improved immune-related readouts and, in some studies, lower respiratory infection burden or improved vaccine response dynamics. That is meaningful because immune aging is a real functional domain rather than a lab curiosity. It is still not the same as showing a general caloric-restriction mimic across whole-body aging. Rapalogs currently look more like targeted resilience tools than a broad human anti-aging platform.
There is also a dosage and context problem. The biology that looks attractive at low intermittent exposure can become undesirable when suppression is too deep or chronic. This is why the strongest rapalog case in humans is not "take rapamycin and become calorie restricted without dieting." It is "mTOR modulation may improve selected late-life functional domains if the schedule is engineered well enough."
Spermidine, Urolithin A, and NAD-Adjacent Compounds: Real Signals, Narrow Claims
Spermidine remains attractive because it is linked to autophagy and cell-maintenance pathways, and some human studies suggest cognitive or cardiometabolic movement. The evidence quality still varies. Reviews published in 2024 and 2025 remain cautiously positive, not definitive. This is a recurring pattern in the mimetics space: a plausible mechanism, a few encouraging human endpoints, and a much larger narrative built on the hope that those endpoints generalize into systemic aging control.
Urolithin A may be one of the cleaner examples of how to read the field properly. Human studies suggest effects on mitochondrial or muscle-related measures, and more recent work reported improvement in cardiovascular health biomarkers. That is a legitimate translational signal. It is not proof that urolithin A reproduces calorie restriction across the organism. It means a compound may improve a domain that calorie restriction also touches, which is a weaker and more defensible claim.
NAD-boosting strategies have the same interpretive trap. The pathway logic is attractive. Human results have generally been mixed, modest, or endpoint-limited. If a compound improves one metabolic or exercise-related readout without producing broader durable functional gains, that does not make it a calorie-restriction mimetic in any strong sense.
What Actually Works in Humans
The answer depends entirely on the level of the claim.
- If the claim is broad calorie-restriction replacement: nothing has earned that status in humans.
- If the claim is narrower metabolic improvement in a disease-linked context: metformin works, but that is not the same thing as proven longevity benefit.
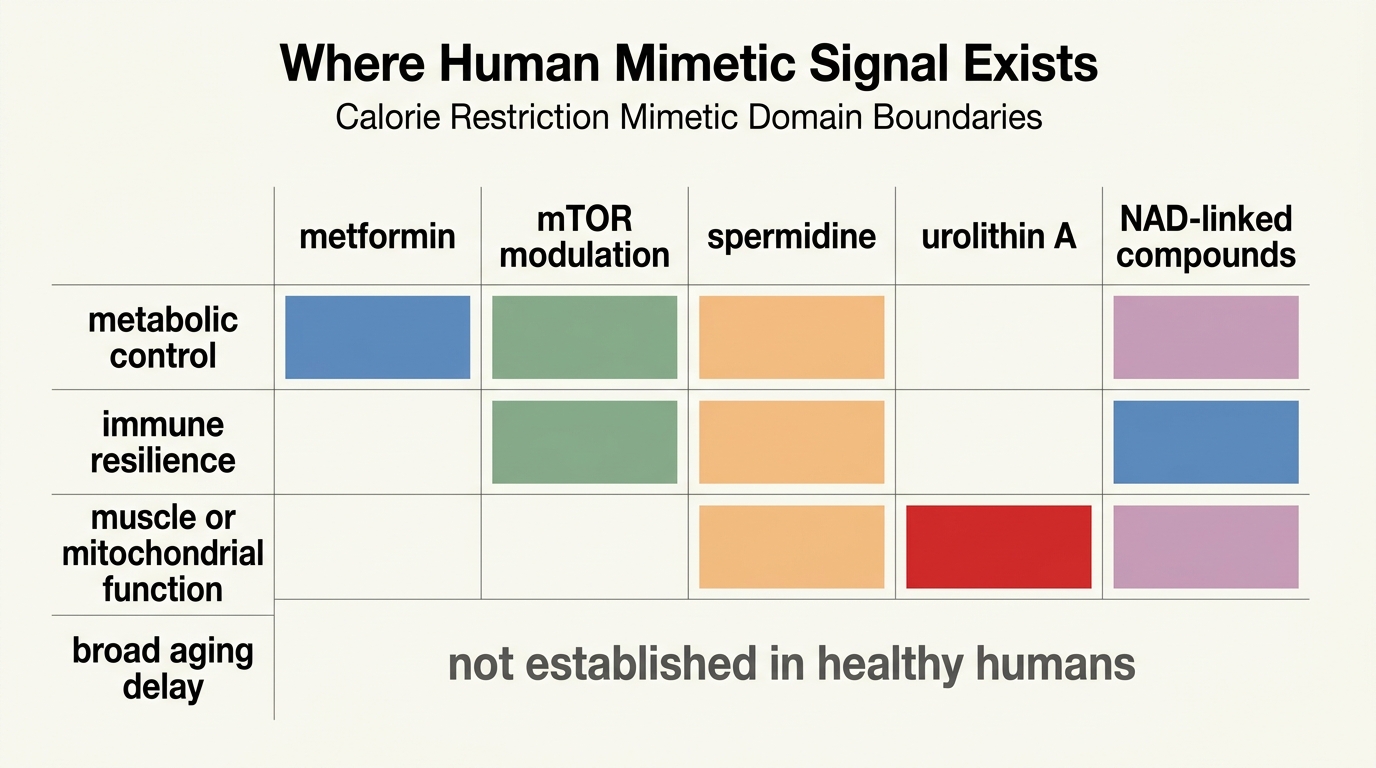
- If the claim is selective late-life functional enhancement: low-dose mTOR-pathway inhibition has some of the most credible domain-specific human evidence.
- If the claim is mitochondrial or autophagy-linked improvement on bounded endpoints: urolithin A and spermidine look plausible, but the case remains narrower than the marketing language around them.
This distinction is the central correction the field still needs. Several compounds work in the modest sense that they move something relevant in humans. Very few work in the strong sense implied by the word mimetic when it is heard as "calorie restriction in pill form." The first is evidence. The second is overreach.
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | Calorie restriction itself improves multiple cardiometabolic and inflammatory markers in controlled human trials. |
| Known | Metformin, low-dose mTOR-pathway inhibition, spermidine, and urolithin A each have some human endpoint signal, but those signals are domain-specific and uneven. |
| Inferred | No single compound is likely to reproduce the full systems effect of calorie restriction because calorie restriction itself operates across multiple interacting pathways. |
| Unknown | Which intervention, dose schedule, or combination strategy can deliver durable aging-related benefit in broadly healthy humans without unacceptable tradeoffs over long follow-up. |
What Would Count as a Real Breakthrough
A serious breakthrough would need more than biomarker movement. It would show durable functional benefit in humans, measured across outcomes that matter outside the lab. Those could include immune resilience, muscle function, cardiometabolic burden, cognitive durability, or clinically meaningful multi-domain aging composites. The intervention would also need a credible safety story under repeated use.
That is where many mimetic narratives still break. They start with a mechanistic diagram, pass through animal lifespan work, touch a human biomarker, and then leap directly to consumer use. The missing middle is precisely where responsible translation lives.
For LifeMeter readers, the practical conclusion is conservative but not dismissive. The mimetics field is not empty. It is just narrower than its public image. If the question is whether any intervention already reproduces calorie restriction's human effects in a pill, the answer is no. If the question is whether several compounds now show real, bounded human effects on aging-relevant systems, the answer is yes. The mistake is pretending those are the same claim.
Further Reading Inside the Site
This article connects directly to Metformin as a Longevity Drug: Evidence vs Assumption, NAD+ Restoration: Mechanism, Hype, and Clinical Signal, and GLP-1 Drugs as a Longevity Bridge. Together they separate serious translational candidates from category-level hype.
Source List
Kraus WE, et al. 2 years of calorie restriction and cardiometabolic risk (CALERIE phase 2). Lancet Diabetes Endocrinol. 2019.
Dorling JL, et al. Effect of 2 years of calorie restriction on liver biomarkers: results from the CALERIE phase 2 randomized controlled trial. Eur J Nutr. 2021.
Justice JN, et al. Caloric restriction intervention alters specific circulating biomarkers of the senescence-associated secretome. J Gerontol A. 2024.
Zhou J, et al. Metformin: An Old Drug with New Applications. Int J Mol Sci. 2018.
Mannick JB, et al. Targeting the biology of ageing with mTOR inhibitors to improve immune function in older adults. Lancet Healthy Longev. 2021.
Arthur R, et al. A review on polyamines as promising next-generation neuroprotective and anti-aging therapy. Eur J Pharmacol. 2024.
Zou M, et al. The memory- and cognition-facilitating effects of spermidine in aging and aging-related disorders. Ageing Res Rev. 2025.
Liu S, et al. Urolithin A provides cardioprotection and mitochondrial quality enhancement preclinically and improves human cardiovascular health biomarkers. iScience. 2025.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.