Functional Age vs Chronological Age: Which Matters More?
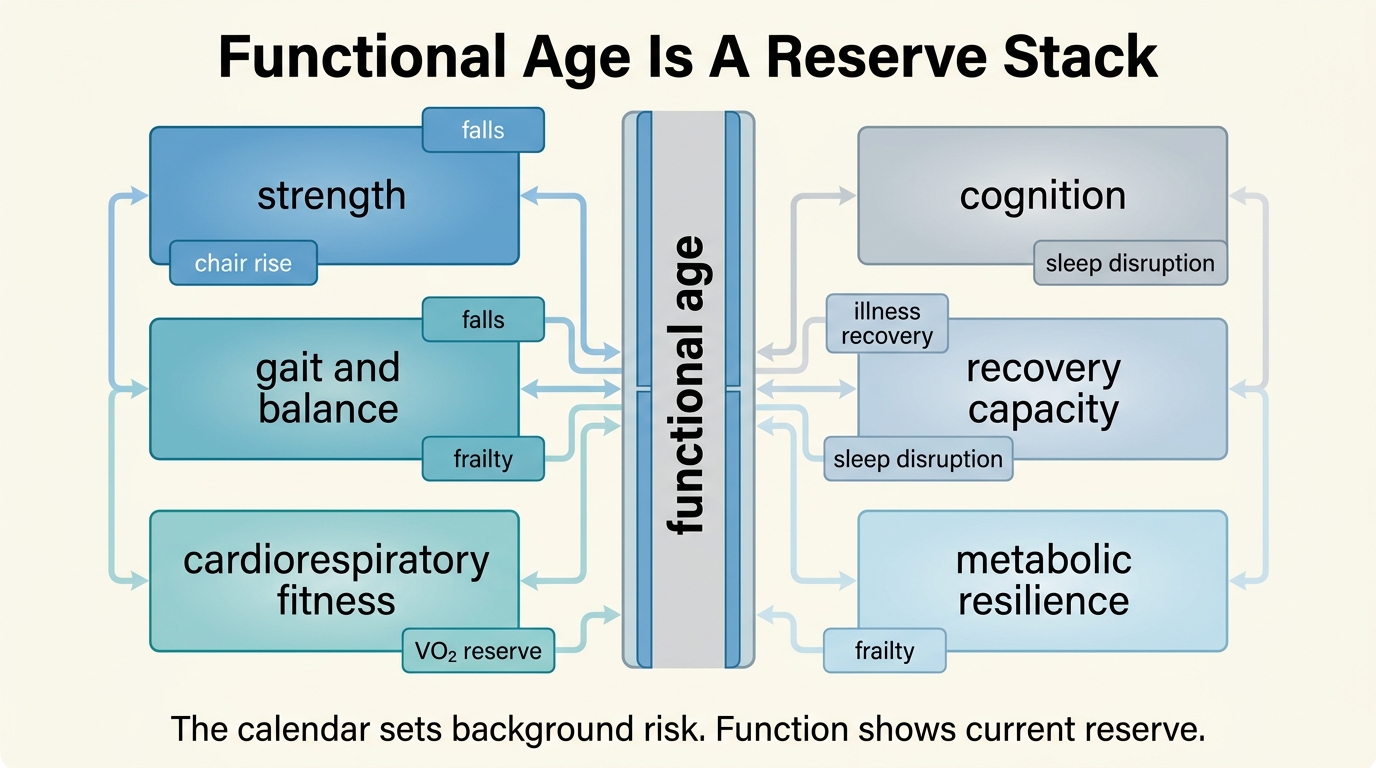
The calendar is blunt. Two people can be the same chronological age while differing sharply in strength, gait speed, cardiorespiratory fitness, recovery capacity, and cognitive resilience. That is why functional age so often feels more real than the birth date. The mistake is to turn that insight into a false choice. Chronological age still matters. Functional age often matters more for current risk and near-term decision quality.
Chronological age is a background risk variable. It captures cumulative exposure time. It remains one of the strongest predictors in epidemiology because many diseases, repair failures, and reserve losses increase with years lived. But the calendar does not tell you how that risk is being expressed inside a specific person right now. It does not tell you whether the person in front of you has preserved reserve or is already moving into a narrow physiological corridor.
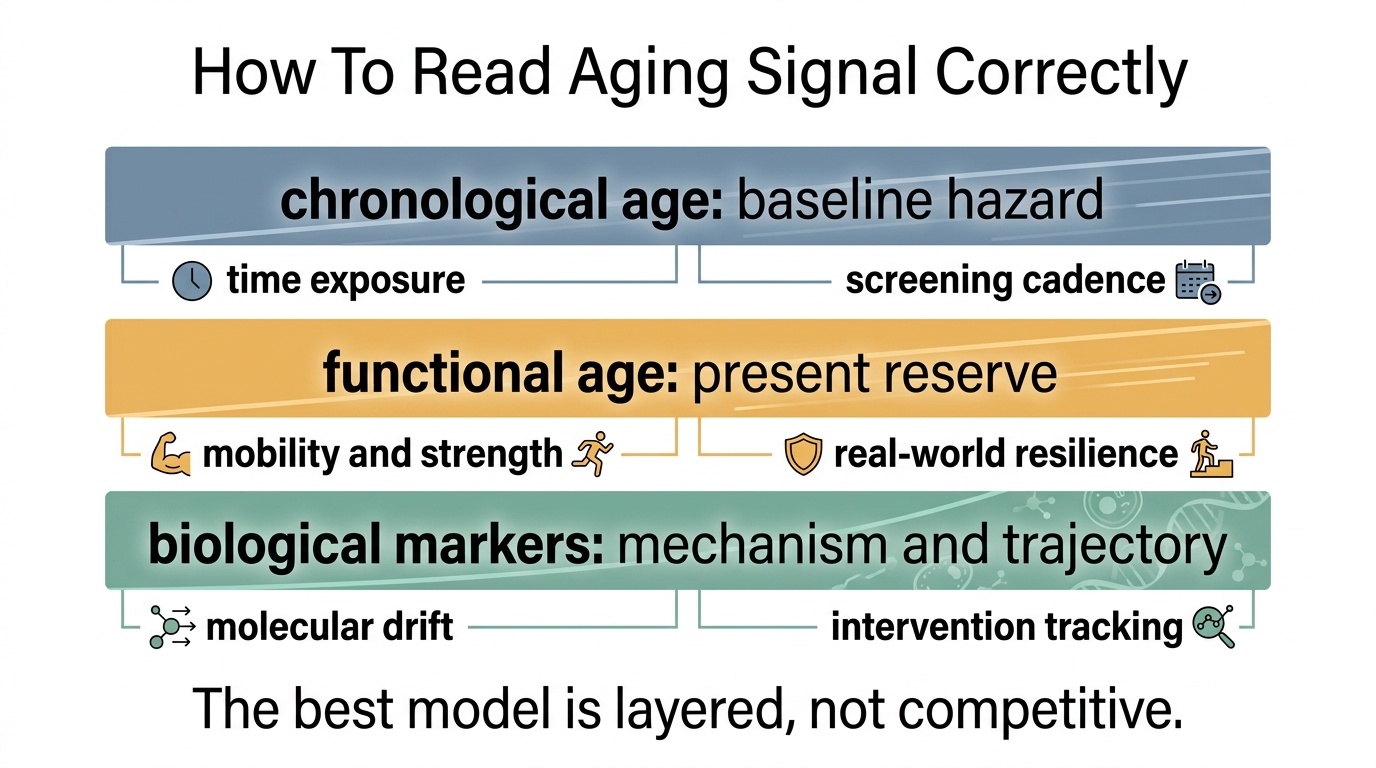
Core thesis: chronological age is indispensable for population-level risk framing, trial design, and actuarial expectation. Functional age is often more decision-relevant for the individual because it captures reserve, mobility, strength, and real-world resilience. The strongest model is layered: use the calendar for baseline risk, function for current state, and biological markers for mechanism and trajectory.
Why Functional Age Usually Feels Truer
Most people do not experience aging as a birthday count. They experience it as a change in what the body can still do. Can you climb stairs without strategic planning. Can you carry load, recover from illness, maintain lean mass, tolerate travel, preserve sleep quality, and retain aerobic range. Those are functional questions, and they often explain daily aging reality better than the calendar does.
This is also why functional markers repeatedly predict meaningful outcomes. Slower gait speed, weaker grip strength, lower cardiorespiratory fitness, and poorer composite physical-performance scores are not cosmetic findings. They map to falls, disability, hospitalization, and mortality risk. They are useful because they measure expressed reserve rather than abstract possibility.
What Chronological Age Still Does Better
The backlash against chronological age sometimes overcorrects. Time remains biologically relevant because damage exposure, clonal expansion, cumulative inflammation, vascular wear, immune remodeling, and cancer risk do not occur outside time. Age is still a strong prior. If two people have the same functional profile today but one is fifteen years older, the older person usually carries more background vulnerability and a narrower margin for error.
Chronological age is therefore still useful in three places. It anchors base-rate expectations. It helps compare like with like in clinical trials and screening policy. It also keeps longevity discourse honest by preventing every high-functioning outlier from being mistaken for a proof that aging risk can be ignored. Functional age may win the state question. The calendar still matters for the hazard question.
Where Biological Clocks Fit
Biological-age clocks entered this debate because they promise something between the calendar and function. In principle they can detect molecular drift before overt decline appears. That is useful. It is not enough to resolve the hierarchy by itself. A clock can move without a corresponding change in strength or endurance. A person can also function well while carrying molecular risk that has not yet become visible in daily performance.
The right interpretation is complementarity, not replacement. Clocks can help estimate trajectory. Functional markers help estimate present reserve. Chronological age helps place both inside expected risk gradients. A serious longevity workflow uses all three and refuses to let any one of them dominate without cross-checks.
What Counts As Functional Age In Practice
| Domain | Why It Matters | Main Limitation |
|---|---|---|
| Gait and mobility | Captures integrated neuromuscular, cardiovascular, and balance reserve. | Can look normal until challenge rises or decline becomes more advanced. |
| Strength | Reflects muscle reserve, frailty risk, and recovery capacity. | Single tests can miss asymmetry and endurance limitations. |
| Cardiorespiratory fitness | Strongly tracks resilience, aerobic reserve, and mortality risk. | Best measurement often requires formal testing. |
| Composite performance tools | Bundle balance, chair rise, and walking into a more realistic reserve picture. | Scores can compress high-functioning people together. |
| Cognition and recovery | Functional aging is not only musculoskeletal. Executive control and resilience matter. | Measurement is less standardized in routine longevity practice. |
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | Chronological age remains a strong population-level risk variable because many disease and mortality hazards rise with cumulative exposure time. |
| Known | Functional markers such as gait speed, grip strength, cardiorespiratory fitness, and physical-performance batteries predict adverse outcomes and often capture current reserve better than the calendar alone. |
| Known | Biological markers and clocks can add mechanistic and trajectory information, but they do not eliminate the need to check whether a person is actually functioning well. |
| Inferred | The best operational model for longevity decisions is layered rather than singular: calendar for baseline risk, function for present state, and molecular markers for trajectory. |
| Unknown | Which integrated scoring systems will become reliable enough for routine clinical use without collapsing complex reserve into another misleading single number. |
Why This Changes Intervention Logic
If functional age matters more for real-world reserve, then interventions should be judged against function, not only against weight loss, lab movement, or clock novelty. That point is central to GLP-1 and Functional Age: When Weight Loss Helps Longevity and When It Hurts. A therapy that improves one biomarker while worsening lean mass, strength, or aerobic capacity may produce a cleaner dashboard and a weaker organism.
The same logic sharpens prevention. A person with preserved function at an older chronological age should not be treated as metabolically identical to a younger person with low reserve, sedentary capacity, and unstable recovery. Functional age changes how aggressively one should prioritize resistance training, protein adequacy, fall prevention, mobility work, sleep repair, or medical screening cadence.
The Better Question
The goal is not to decide whether functional age or chronological age matters in absolute terms. The better question is which one answers the decision in front of you. If you are estimating disease incidence at scale, the calendar is indispensable. If you are deciding whether a specific person is robust, frail, or functionally declining despite decent labs, functional age often carries more signal. If you want to understand mechanism or trajectory, biological markers matter as the third layer.
That is the durable framework. Do not collapse aging into birthdays. Do not collapse it into one clock score either. Ask what the person can still do, how much reserve remains, and how the molecular and clinical picture lines up behind that performance.
Further Reading Inside The Site
This article connects directly to Biological Age Clocks as Decision Tools, GLP-1 and Functional Age, and The 2026 Dyslipidemia Rewrite. Together they show why the most useful longevity metrics are those that improve real decisions rather than only producing cleaner abstractions.
Source List
Studenski S, Perera S, Patel K, et al. Gait speed and survival in older adults. JAMA. 2011.
Nunez-Cortes R, Del Pozo Cruz B, Gallardo-Gomez D, et al. Handgrip strength measurement protocols for all-cause and cause-specific mortality outcomes in more than 3 million participants. Clinical Nutrition. 2022.
Laukkanen JA, Isiozor NM, Kunutsor SK. Objectively assessed cardiorespiratory fitness and all-cause mortality risk. Mayo Clinic Proceedings. 2022.
Kameniar K, Mackintosh S, Van Kessel G, Kumar S. The psychometric properties of the Short Physical Performance Battery to assess physical performance in older adults. Journal of Geriatric Physical Therapy. 2024.
Viccaro LJ, Perera S, Studenski SA. Is timed up and go better than gait speed in predicting health, function, and falls in older adults?. Journal of the American Geriatrics Society. 2011.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.