Hallmarks of Aging Revisited: What Changed Since 2013
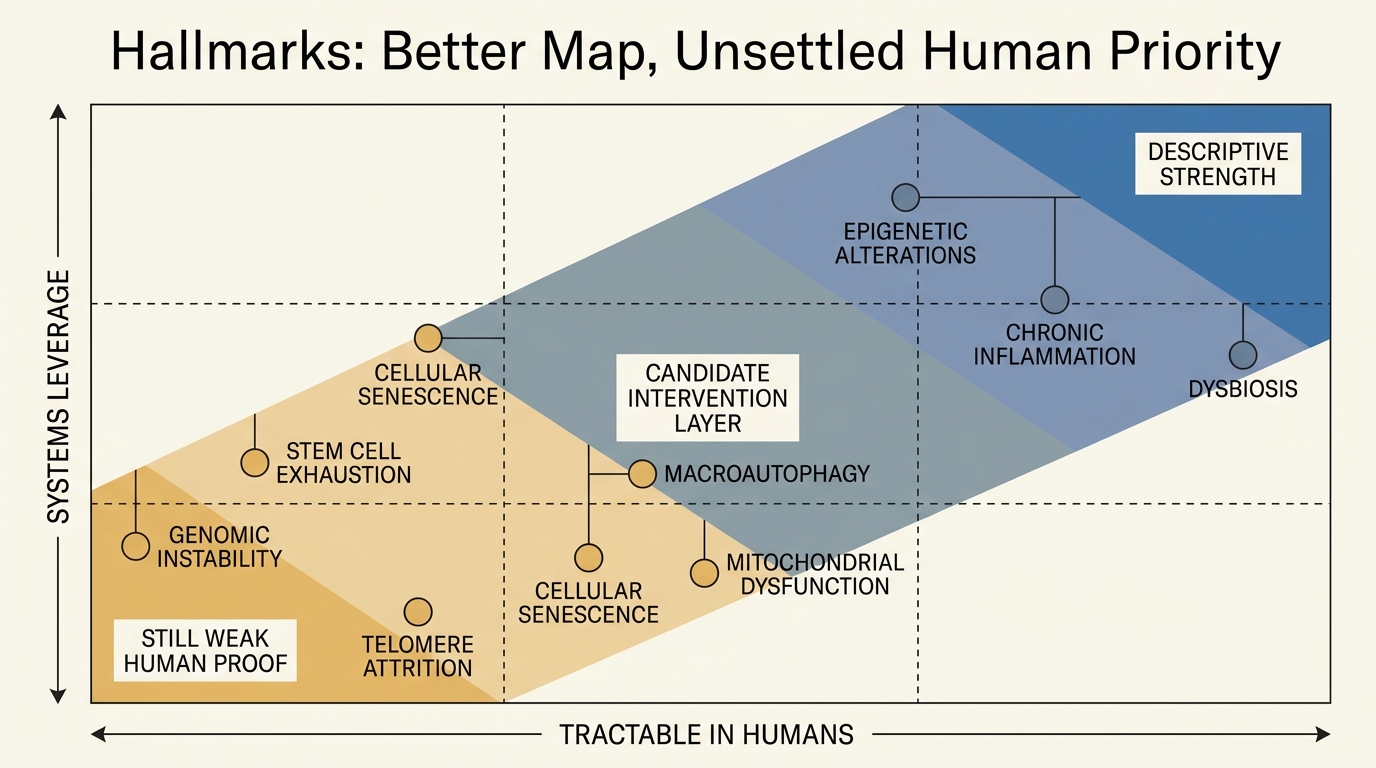
The hallmarks framework still matters because aging research needs a systems map before it can justify an intervention stack. The map is better than it was in 2013. The ranking problem is still not solved.
The 2013 Cell paper became foundational because it gave the field a disciplined way to compare mechanisms that had usually been discussed in isolation. Instead of choosing one grand cause of aging, it asked whether a process appeared during normal aging, whether intensifying it accelerated decline, and whether attenuating it slowed decline or improved healthy lifespan. That did not settle causality. It made the debate more rigorous.
What Changed Since 2013
The 2023 expansion mattered because it tightened what the map is expected to do. The field moved from describing recurring damage patterns toward asking which failures are upstream enough, measurable enough, and tractable enough to anchor real human intervention. That harder question remains open.
The 2013 Cell paper became canonical because it did something simple and hard at the same time. It turned a field full of rival causal stories into a framework with common criteria. A hallmark had to appear during normal aging, experimental intensification had to accelerate aging, and experimental attenuation had to slow aging or extend healthy lifespan. That standard did not prove that every hallmark was equally upstream. It did make the debate much more disciplined.
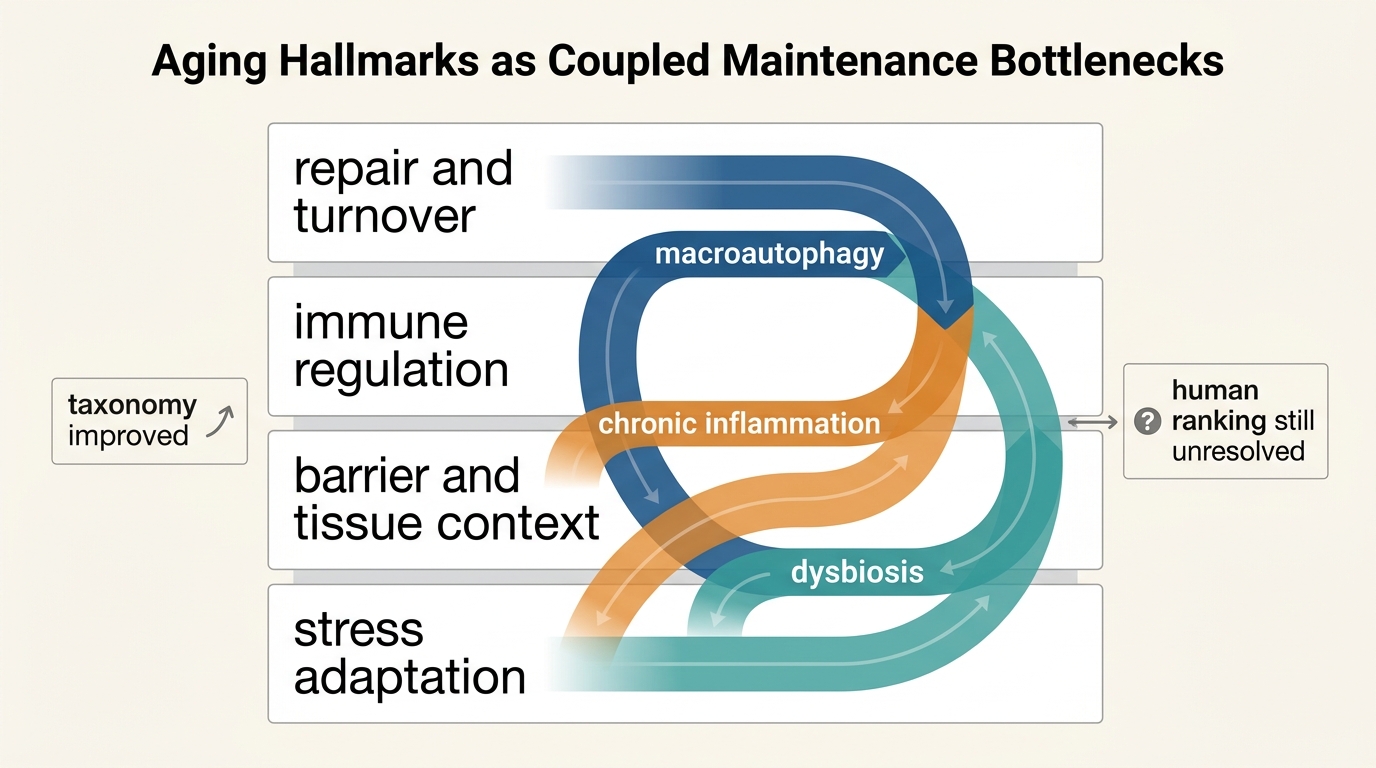
Core thesis: the real shift since 2013 is not only that the list expanded from nine hallmarks to twelve. The stronger shift is that aging is now framed more explicitly as a coupled maintenance failure. That makes the framework biologically stronger while making clinical prioritization harder.
What The 2013 Paper Established
The original paper proposed nine hallmarks: genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, deregulated nutrient sensing, mitochondrial dysfunction, cellular senescence, stem cell exhaustion, and altered intercellular communication. It also organized them into primary, antagonistic, and integrative layers. That architecture made it easier to discuss upstream damage, compensatory responses, and organism-level failure without insisting that one process had to explain everything.
That organizational step mattered more than many readers realized. Aging biology had no shortage of mechanisms before 2013. It lacked a durable way to compare them. The hallmarks paper gave the field a common language for asking whether an intervention was acting on genome maintenance, nutrient signaling, senescent burden, stem-cell function, or tissue communication. A framework that allows cleaner disagreement is often more valuable than a theory that pretends to settle the matter.
Still, the 2013 map reflected the evidence structure of that period. Autophagy was mostly nested inside proteostasis. Inflammation was discussed, but chiefly through altered intercellular communication. The microbiome appeared as context rather than as a core node. Those placements were understandable at the time. They were not the end state.
What The 2023 Expansion Actually Changed
The 2023 revision expanded the list to twelve by adding disabled macroautophagy, chronic inflammation, and dysbiosis. That was not cosmetic inflation. It reflected the view that these processes had become too consequential and too mechanistically distinct to remain buried inside broader categories.
Disabled macroautophagy became a stand-alone hallmark because general proteostasis had become too broad. Protein quality control, organelle recycling, stress response, and intracellular waste handling are related, but they are not interchangeable. A cell can retain some proteostatic capacity while still failing to recycle damaged components at a level that matters for long-term resilience. Giving macroautophagy its own category forces more precise intervention claims.
Chronic inflammation moved from background condition to explicit driver because the literature increasingly supports bidirectional causality. Aging processes generate inflammatory tone, yet persistent inflammatory signaling also worsens senescence, stem-cell impairment, tissue remodeling, and organ dysfunction. Treating inflammation as a downstream byproduct no longer fits the full evidence pattern.
Dysbiosis entered the formal list because the field widened from cell-intrinsic aging toward host-system aging. Barrier integrity, microbial composition, immune education, and metabolite handling all matter for how aging is expressed. The microbiome literature still has substantial causality gaps in humans, but the framework changed because recurrent age-linked disruption and systemic interaction became too prominent to leave on the margins.
The Deeper Shift Was From Damage Catalog To Maintenance Logic
The revised framework is most useful when read as a maintenance map rather than as a larger checklist. Aging is not only the accumulation of defects. It is also the failure of systems that preserve turnover, stress response, tissue context, and multi-scale homeostasis.
This is where the 2021 hallmarks-of-health paper matters. That paper did not replace the hallmarks of aging. It supplied a mirror image. If health depends on preserved boundaries, robust stress handling, and functional homeostasis over time, then aging can be described as the progressive collapse of those maintenance functions. The result is an intervention map that is better aligned with real biological tradeoffs. A therapy can move a biomarker while still failing to restore the maintenance architecture that produced the biomarker in the first place.
The practical consequence is easy to miss. Once the field shifts toward maintenance logic, prioritization becomes harder rather than easier. Broad categories such as inflammation or mitochondrial dysfunction may touch many outcomes, but that alone does not tell us whether they are primary drivers in a given tissue, late markers of deeper injury, or useful but incomplete control points. A more mature framework increases biological realism while reducing the temptation to pretend there is one obvious master node.
The Unsolved Problem Is Priority, Not Taxonomy
Separating macroautophagy, inflammation, and dysbiosis matters because each one changes how intervention claims should be evaluated. If autophagic competence is poor, a therapy that depends on intracellular cleanup may fail for reasons that have little to do with its headline mechanism. If chronic inflammation is acting as a propagating driver rather than a passive marker, then reducing upstream damage without addressing inflammatory state may leave the system unstable. If dysbiosis shapes immune tone and barrier function, then a purely cell-intrinsic intervention may underperform in whole organisms even when it looks elegant in narrow models.
But the stronger taxonomy does not solve ranking. Some hallmarks are easier to measure than to repair. Some are broad enough to organize thinking but too composite to serve as clean drug targets. Some interventions may improve one layer while worsening another through tradeoffs in cancer control, immune tone, growth signaling, or tissue specificity. That is why the mature reading of the hallmarks framework is less triumphalist than many summaries suggest. It is a better decision scaffold, not a resolved human intervention stack.
What Did Not Change
The revision did not abolish the older framework. Genomic instability, telomere attrition, epigenetic change, nutrient-sensing dysregulation, mitochondrial dysfunction, senescence, stem-cell exhaustion, and altered intercellular communication still sit near the center of the field. The problem is not that the 2013 framework became wrong. It became coarser than the field now requires.
The expansion also did not make every hallmark equally tractable. Some nodes are easier to measure than to repair, and some look clinically attractive only because they are downstream enough to move quickly on biomarkers. The stronger the framework becomes as a map, the easier it is to see that a named hallmark is not the same thing as a validated human leverage point.
It also remains descriptive. The hallmarks framework is excellent for organizing mechanisms and for explaining why single-pathway triumphalism usually fails. It is much weaker as a guide to human leverage points. Some hallmarks may be more upstream than others. Some may be easier to measure than to modify. Some may respond in biomarkers without translating into meaningful function. The framework clarifies the questions. It does not answer them by itself.
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | The 2013 Cell paper proposed nine hallmarks and set explicit criteria for what should count as a hallmark of aging. |
| Known | The 2023 expansion increased the count to twelve by naming disabled macroautophagy, chronic inflammation, and dysbiosis as stand-alone hallmarks. |
| Known | The 2021 hallmarks-of-health framework emphasized maintenance functions such as compartmentalization, homeostasis over time, and stress response. |
| Inferred | The field is increasingly using the hallmarks framework as an intervention-planning tool rather than as a neutral descriptive taxonomy. |
| Unknown | Which combinations of hallmark targets will produce durable functional benefit in humans, and which biomarkers will reliably track that benefit across tissues. |
What This Means For Real Longevity Work
For researchers, the practical implication is that vague anti-aging claims should become harder to defend. Saying that a program addresses aging is not informative enough. The relevant question is whether it changes a specific maintenance layer, whether that layer is rate-limiting in the tissue or disease context at issue, and what compensating risks appear when the same pathway is pushed hard.
For technically literate readers, the practical lesson is restraint. A stronger mechanistic map does not equal clinical closure. The hallmarks framework has improved because it separates more of the biology. That same improvement exposes how much remains unresolved when candidate interventions move from cell systems and animal models into human endpoints.
For LifeMeter, the disciplined takeaway is simple. Aging research did not converge on one master cause after 2013. It converged on a better map of interacting failure modes and maintenance bottlenecks. That is real progress. It is not a shortcut around endpoint evidence, and it does not remove the need to rank which interventions can carry that map into durable human outcomes.
Further Reading Inside The Site
This article connects directly to Extracellular Matrix Aging: The Forgotten Target, Senomorphics vs Senolytics: Slowing vs Removing Damage, and Stem Cell Exhaustion and Replenishment Strategies. Together they show why the updated hallmarks map increasingly points toward coupled maintenance problems rather than isolated lesions.
Source List
López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. The Hallmarks of Aging. Cell. 2013.
López-Otín C, Kroemer G. Hallmarks of Health. Cell. 2021.
López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. Hallmarks of aging: An expanding universe. Cell. 2023.
Qiu Y, Fernández-García B, Lehmann HI, et al. Exercise sustains the hallmarks of health. Journal of Sport and Health Science. 2023.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.