Regulatory Barriers to Anti-Aging Drugs
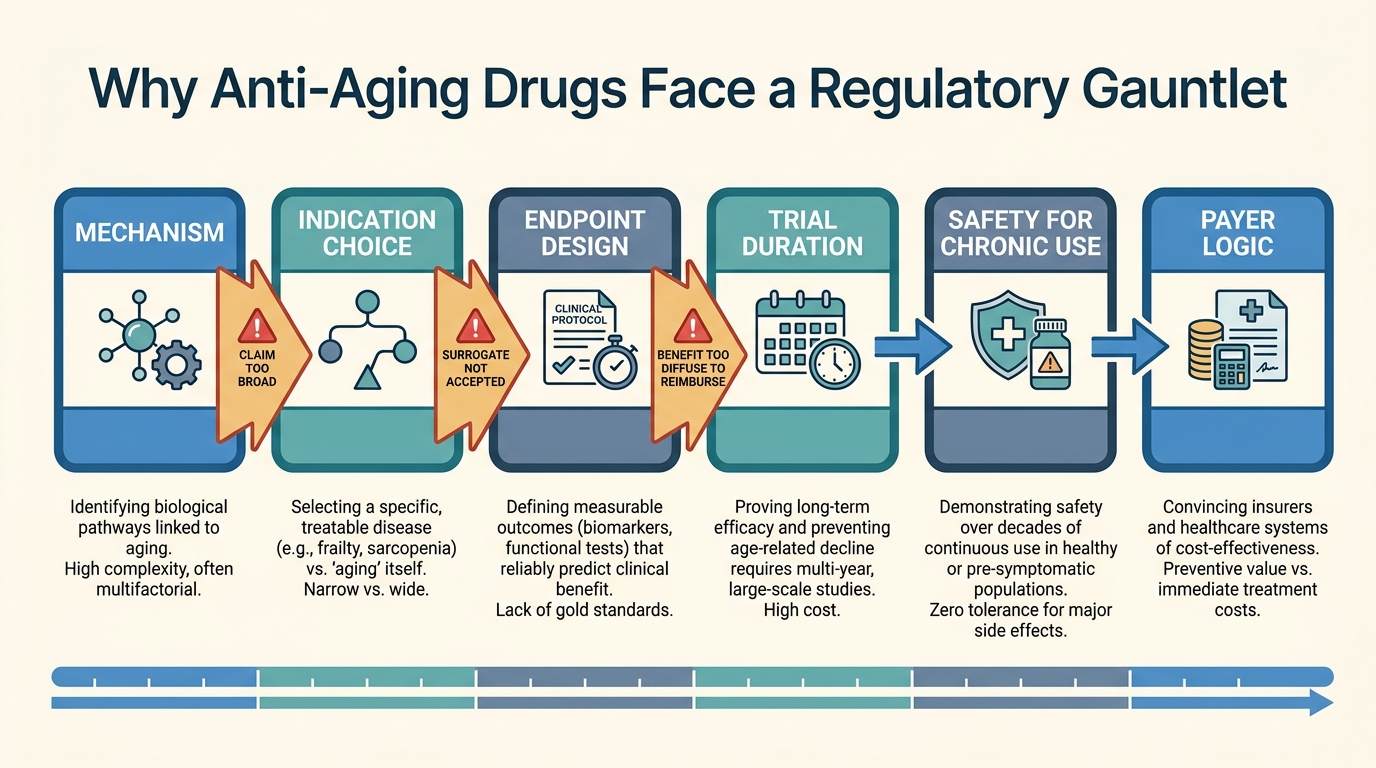
The field often talks as though anti-aging drug progress is mainly a biology problem. Biology is only half the bottleneck. A program also needs an approvable indication, measurable endpoints, follow-up windows that regulators and payers can accept, and a claim structure narrow enough to survive review. Aging itself still resists all four.
The obstacle is not that regulators are irrationally hostile to aging science. The obstacle is that modern drug regulation is built around diseases, symptoms, and patient-relevant outcomes that can be defined with reasonable precision. Aging is broader, slower, and more heterogeneous than that template. A company can show mechanistic plausibility and still have no clean path to approval for an anti-aging label.
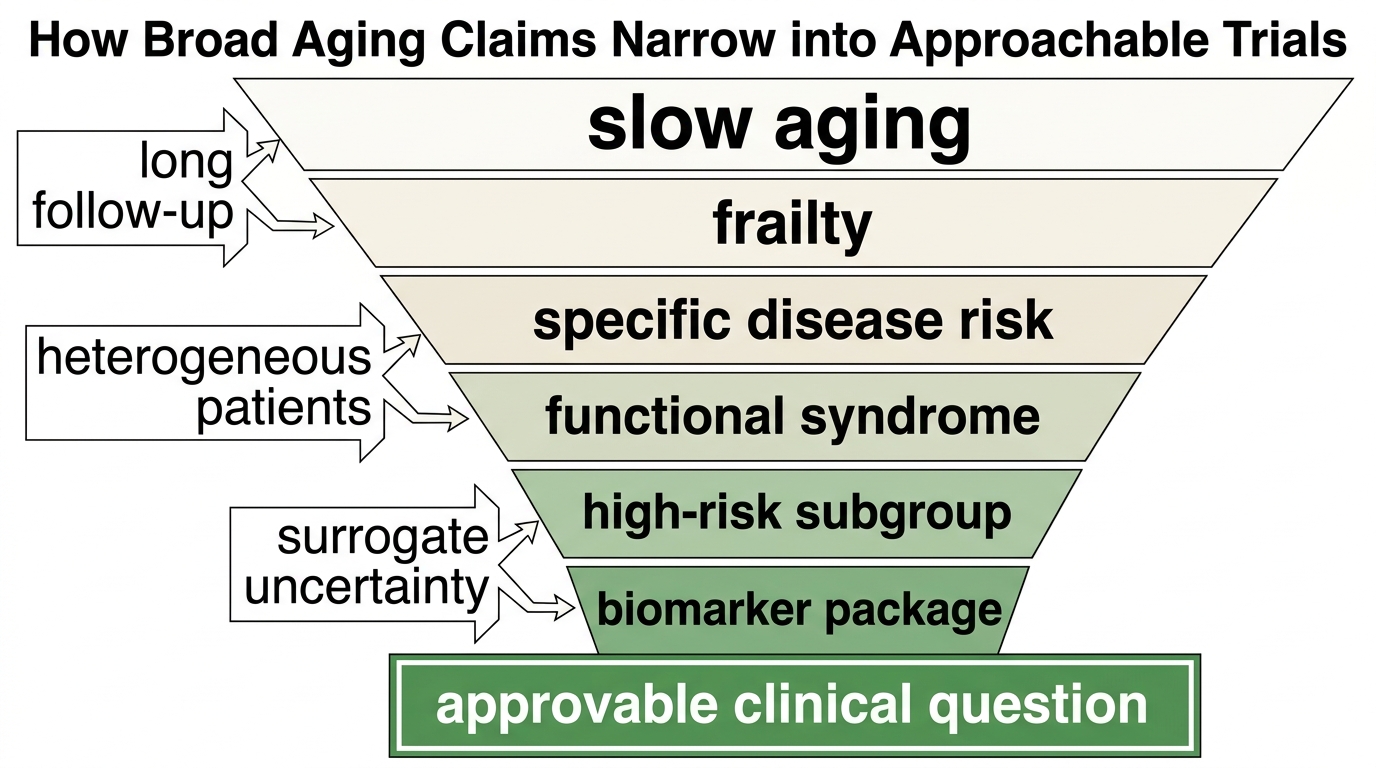
Core thesis: the strongest barrier to anti-aging drugs is not lack of molecular targets. It is the mismatch between the breadth of the aging claim and the narrow logic required for trial design, approval, reimbursement, and post-market use. Serious programs usually have to route through a specific age-related disease, functional syndrome, or high-risk subgroup rather than through aging as a general indication.
Why Aging Is Hard To Regulate As A Drug Target
Drug approval systems are designed to answer a bounded question: does this intervention safely improve a defined condition for a defined population? Aging is not one condition in that sense. It is a distributed rise in vulnerability across tissues, functions, and diseases. That makes it biologically central but regulatorily awkward.
This is why geroscience programs repeatedly gravitate toward proxies such as frailty, multimorbidity risk, osteoarthritis, immune decline, or a single organ system. The narrower frame is not a retreat from ambition. It is often the only way to translate a broad aging hypothesis into an executable clinical program.
The Endpoint Problem Is Structural
An anti-aging claim sounds simple until the endpoint question begins. Lifespan is too slow and too noisy for ordinary trials. Composite disease outcomes can be important, but they require large populations and long follow-up. Biomarkers are faster, yet most remain surrogates rather than accepted stand-ins for broad healthy-aging benefit. Functional endpoints are clinically meaningful, but they often vary with training, motivation, local context, and comorbidity load.
The result is a narrow funnel. A program may have elegant biology, but if it cannot connect that biology to a specific endpoint package that regulators trust, it remains commercially and clinically stalled. This is the same reason investors often overread early clock, omics, or inflammatory data. A biomarker shift is evidence. It is not automatically an approvable claim.
Trial Duration And Safety Requirements Work Against Broad Claims
Aging interventions are usually pitched for long use in older adults who may already carry competing diseases, polypharmacy, and lower physiologic reserve. That immediately raises the safety bar. A therapy that might be tolerable in a short oncology window can look very different if the intended use is chronic prevention across large populations.
Duration matters for efficacy as well. If the hypothesis is that a drug slows the rate of downstream pathology, the trial may need enough time to show a real difference in events or function. That creates a capital problem, but it is also an evidence problem. The field wants fast readouts because long studies are expensive. Regulators need enough follow-up to distinguish temporary biomarker movement from durable patient benefit.
Reimbursement Quietly Shapes What Can Reach Patients
Even if a regulator accepted a broad healthy-aging logic, payers would still ask who qualifies, which outcome matters, how long treatment should continue, and what expenditure it offsets. That is another reason disease-routed programs dominate. Reimbursement systems are better at pricing avoided hospitalization, delayed progression, or preserved function in a defined cohort than at pricing a diffuse promise of slower biological aging.
This does not mean aging-targeted medicine is impossible. It means first approvals are more likely to arrive under narrower labels that can later expand if the evidence base compounds. The market frequently talks as though the first anti-aging winner will arrive as a category-defining umbrella drug. A more plausible path is a series of condition-specific approvals that gradually prove pieces of the aging thesis.
What This Means For The Pipeline
- Expect disease-adjacent entry points. Programs aimed at fibrosis, immune aging, frailty, sarcopenia, or high-risk metabolic populations fit the current system better than a universal aging label.
- Treat biomarkers as trial tools, not verdicts. They are useful for enrichment, dose selection, and mechanism. They rarely settle approval on their own.
- Watch for endpoint discipline. The strongest teams are explicit about what they are trying to improve, for whom, and over what time window.
- Discount broad category rhetoric. A platform that claims to reverse aging everywhere is usually describing aspiration, not an approvable development plan.
- Follow reimbursement logic early. A program with no credible payer story often has no credible scale story either.
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | Modern drug regulation is built around defined indications and patient-relevant outcomes rather than around a general claim of slowing aging across the entire organism. |
| Known | Broad anti-aging endpoints such as lifespan or global healthspan are difficult to evaluate in conventional trials because they require long follow-up, large cohorts, and careful control of competing risks. |
| Known | Most biomarkers proposed for aging still function better as enrichment or mechanistic tools than as accepted surrogate endpoints for a broad anti-aging claim. |
| Inferred | The first durable commercial wins in geroscience are more likely to come through narrower disease or function labels than through approval of aging itself as a single indication. |
| Unknown | Whether regulators and payers will eventually accept a standardized endpoint package that is broad enough to support a true anti-aging label rather than a collection of disease-adjacent claims. |
The Useful Reading For LifeMeter Readers
The practical lesson is not cynicism. It is calibration. A company can have serious science and still be years away from a pathway that can survive development, review, and reimbursement. When a longevity program sounds exciting, the next question is not only what the mechanism does. The next question is what exact claim could be approved if the data were positive.
That is why regulatory friction belongs inside any honest anti-aging forecast. It is not external bureaucracy layered on top of science. It is part of the translation problem itself. The pipeline will mature when teams can connect mechanism, endpoint, safety, label, and payer logic into one coherent package rather than treating regulation as a final hurdle after discovery.
Further Reading Inside The Site
This article connects directly to Metformin as a Longevity Drug: Evidence vs Assumption, AI-Designed Longevity Drugs: Early Successes and Limits, and Longevity Clinics: Science, Protocols, and Variability. Together they show why plausible biology still needs a translation pathway that can survive real-world medicine.
Source List
Barzilai N, Cuervo AM, Austad S. Aging as a Biological Target for Prevention and Therapy. JAMA. 2016.
Justice JN, Kritchevsky SB, Ferrucci L, et al. Frameworks for Proof-of-Concept Clinical Trials of Interventions that Target Fundamental Aging Processes. Journal of Gerontology A. 2018.
Espeland MA, Crimmins EM, Grossardt BR, et al. Clinical Trials Targeting Aging and Age-Related Multimorbidity. Journal of Gerontology A. 2017.
Kaeberlein M. How Healthy Is the Healthy Aging Pipeline?. Nature Aging. 2022.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.