Metformin as a Longevity Drug: Evidence vs Assumption
Metformin has become the default pharmaceutical candidate in mainstream longevity conversation because it combines three rare attributes: decades of clinical use, low cost, and a biologically plausible link to several pathways implicated in aging. That makes it a serious candidate. It does not make it a demonstrated human longevity drug.
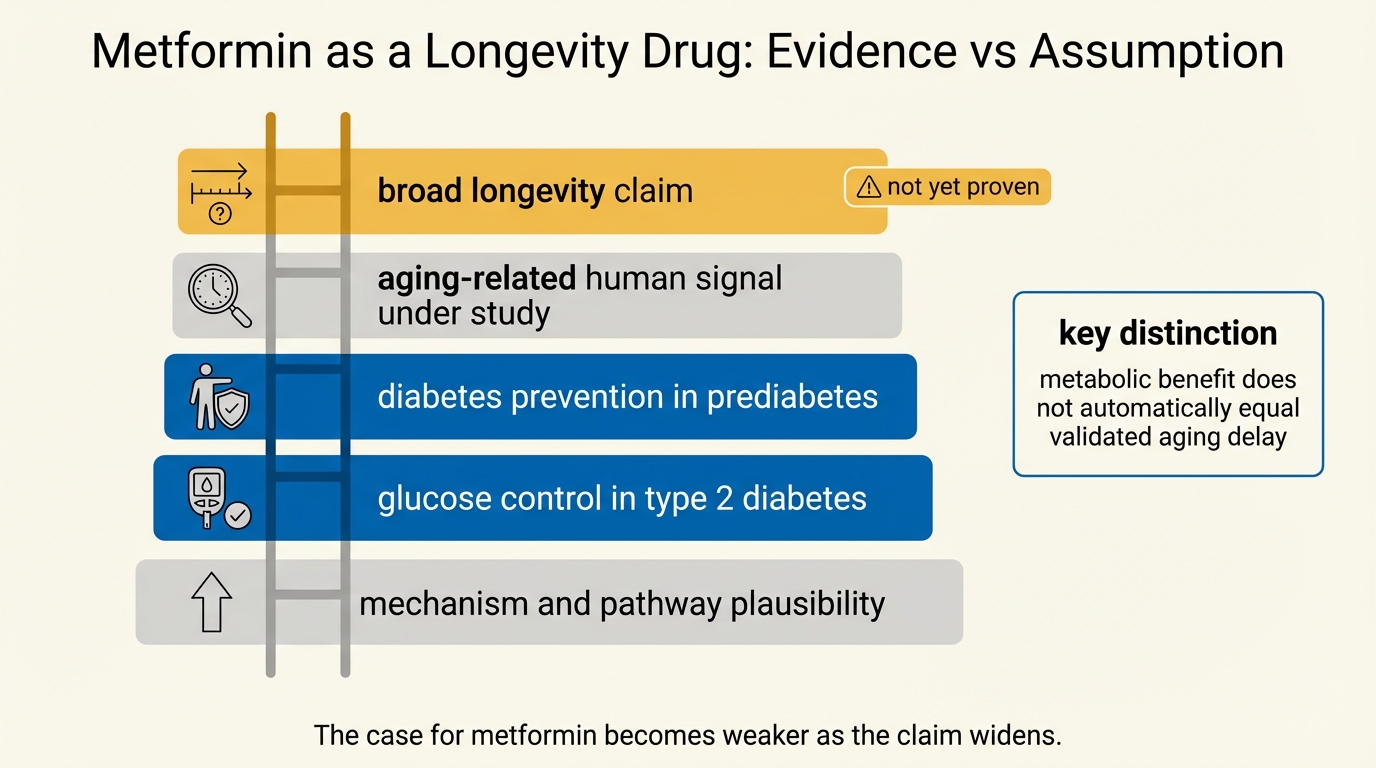
The distinction matters because the argument often jumps over its weakest step. Established fact: metformin reduces progression to type 2 diabetes in high-risk populations, has durable weight and glycemic effects in some groups, and remains one of the most studied drugs in metabolic medicine. Established fact: aging biology contains mechanisms metformin could plausibly influence, including AMPK signaling, nutrient sensing, inflammation, and mitochondrial stress responses. The stronger claim, that metformin broadly slows human aging in otherwise healthy adults, is still an inference under active test.
Core thesis: metformin is a credible geroscience candidate because it has strong metabolic evidence, a known safety profile, and plausible overlap with aging pathways. The human evidence still supports a narrower conclusion: metformin clearly helps some high-risk metabolic populations, may improve selected aging-relevant outcomes, and has not yet earned the status of a general-purpose longevity drug.
Why Metformin Entered The Longevity Conversation
Metformin did not enter aging research through branding. It entered because several features made it unusually testable. It lowers hepatic glucose production, improves insulin sensitivity in many settings, activates AMPK-related signaling, and appears to intersect with inflammation, oxidative stress, and nutrient-sensing pathways that also appear in aging frameworks. Barzilai and colleagues helped frame the modern geroscience argument: if aging is a risk factor bundle rather than one disease, then a drug that shifts multiple downstream disease risks could be a rational way to target aging biology operationally.
That is the best argument for metformin. It is not that metformin has already shown lifespan extension in humans. It is that the drug sits at the junction of practicality and plausibility. Many stronger mechanistic anti-aging ideas remain preclinical or operationally risky. Metformin is already on the shelf, understood by clinicians, and cheap enough to test at scale.
What Human Trials Actually Support
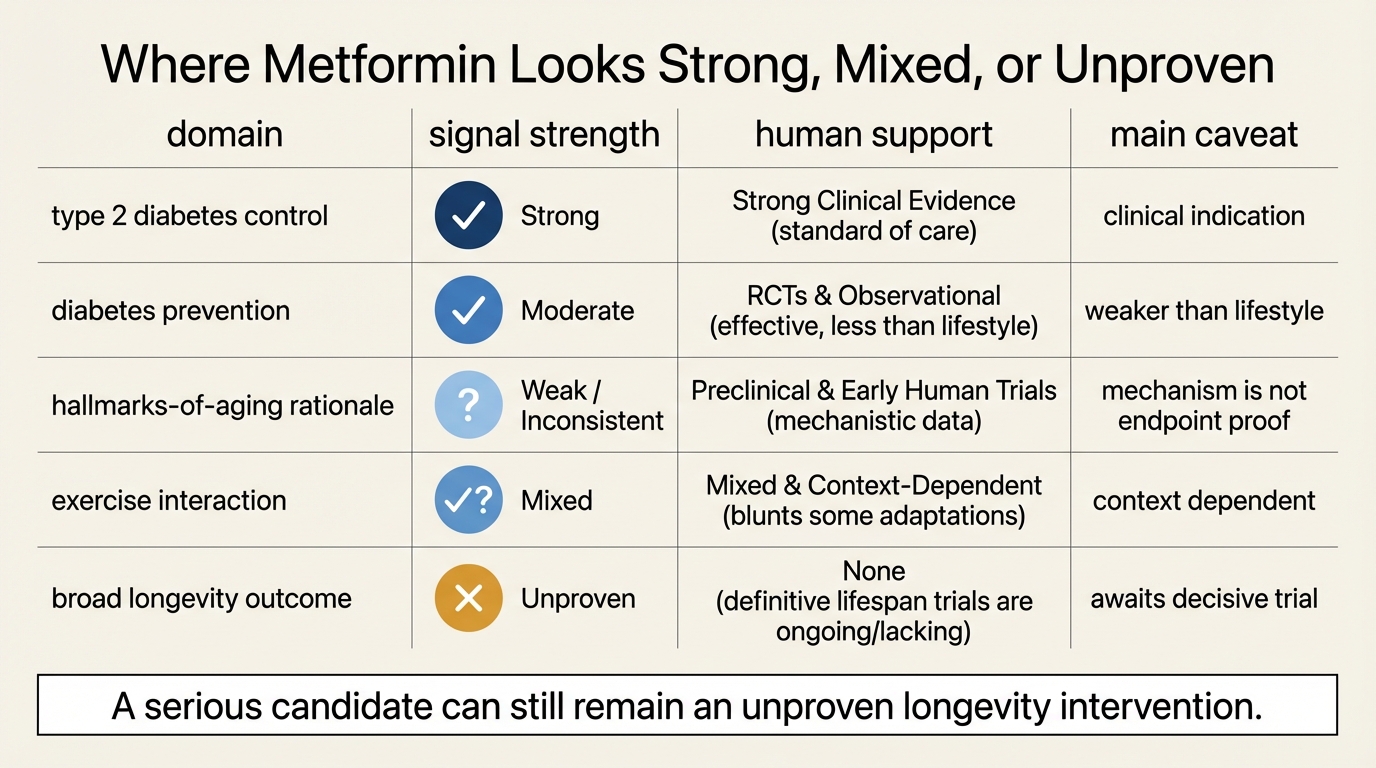
The strongest randomized human evidence still comes from diabetes prevention, not from broad anti-aging endpoints. Across the Diabetes Prevention Program and its long follow-up, metformin reduced diabetes incidence in high-risk adults and continued to show benefit over very long follow-up, although weaker than intensive lifestyle intervention on the original primary endpoint. The 2025 DPP follow-up extended that story to about 21 years and still found reduced diabetes incidence, which matters because it shows durability rather than only a short intervention effect.
That evidence is highly relevant to aging, but it is not identical to longevity proof. Preventing or delaying diabetes reduces one major age-related disease pathway. It does not automatically imply a broad slowing of biological aging across systems. The same caution applies to long-term weight effects in DPPOS. Durable weight reduction can be meaningful, but it is still a partial outcome inside a narrower metabolic population.
Recent frailty-oriented work keeps the case alive while also showing its limits. The 2025 MET-PREVENT randomized trial tested metformin in older adults with probable sarcopenia and prefrailty or frailty. That is exactly the sort of aging-relevant population where a positive signal would matter. The result was not a decisive breakthrough. It adds information, but not closure. Other smaller trials and secondary studies have reported mixed results on gait speed, grip strength, quality of life, and inflammatory markers. The pattern is consistent with a candidate drug that may help some aging-relevant endpoints in some contexts, but not with a universal anti-aging effect already demonstrated.
Where The Case Becomes Too Loose
The slippage usually happens in one of two ways. The first is category inflation. Diabetes prevention, weight effects, and selected frailty or vascular markers are treated as though they already sum to general longevity efficacy. They do not. The second is mechanistic overreach. Because metformin touches pathways that matter in aging, it is easy to talk as though pathway overlap is nearly equivalent to outcome proof. Biology does not work that cleanly.
The caution is not theoretical. Some data suggest metformin can blunt certain exercise-training adaptations, depending on population and endpoint. That matters because a drug meant to support healthy aging cannot be judged only by whether it improves fasting glucose or inflammatory markers in isolation. It also has to be assessed against the interventions older adults already benefit from, especially exercise. A drug that helps one pathway while dulling another adaptation is not disqualified, but it does become harder to treat as a general longevity bridge.
Safety also has to be kept in view. Metformin is comparatively safe, but not free. Gastrointestinal intolerance is common, renal function matters for prescribing, and long-term DPPOS data showed higher rates of low or borderline-low vitamin B12 among metformin users. That is manageable medicine, not a scandal. It does mean the popular story that metformin is almost costless is analytically weak.
What A Serious Longevity Standard Would Require
- Population clarity. Stronger evidence on which non-diabetic or prediabetic older adults actually benefit, rather than treating all midlife and late-life adults as one target.
- Functional outcomes. Durable gains in physical function, frailty progression, cognition, disability, or other clinically meaningful endpoints, not only biomarker movement.
- Intervention comparison. Clear evidence on how metformin interacts with exercise, dietary change, and other standard healthspan interventions.
- Risk accounting. Better long-horizon data on B12 depletion, intolerance, adherence, and the practical tradeoffs of prolonged use in otherwise healthy adults.
- Aging-specific trial design. Studies built to test multisystem age-related outcomes directly, not only to retrofit aging claims onto diabetes trials.
This is why metformin remains interesting. It is one of the few drugs where such a standard is imaginable at all. It is also why current commentary often outruns the literature. The field is still building the bridge from cardiometabolic benefit to aging intervention, not walking across a completed bridge.
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | Metformin reduces progression to diabetes in high-risk adults and has durable metabolic and weight effects in long-term follow-up studies. |
| Known | Metformin overlaps mechanistically with aging-relevant pathways such as AMPK signaling, inflammation modulation, and nutrient sensing. |
| Known | Long-term use can introduce real tradeoffs, including gastrointestinal intolerance and increased risk of low or borderline-low vitamin B12. |
| Inferred | The most defensible near-term use case is selected higher-risk metabolic or frailty-adjacent populations, not blanket anti-aging use in healthy adults. |
| Unknown | Whether metformin meaningfully slows multisystem human aging independent of its established metabolic benefits. |
The Practical Reading For 2026
The honest 2026 position is neither dismissal nor overstatement. Metformin is one of the few repurposed drugs that deserves continued aging-focused study because the cost of testing is low and the biological plausibility is real. It is also still one of the easiest drugs to oversell because the diabetes evidence is strong enough to create false confidence outside the populations where it has actually been proven.
For LifeMeter readers, the useful frame is strict. Metformin is evidence-backed medicine first, a candidate longevity drug second, and a general anti-aging recommendation not yet. If that order is reversed, assumption has replaced evidence.
Further Reading Inside The Site
This article connects directly to Caloric Restriction Mimetics: What Actually Works in Humans, NAD+ Restoration: Mechanism, Hype, and Clinical Signal, and GLP-1 Drugs as a Longevity Bridge. Together they separate serious translational candidates from category-level hype.
Source List
Campbell JM, Stephenson MD, de Courten B, Chapman I, Bellman SM, Aromataris E. Metformin as a Geroprotector: Experimental and Clinical Evidence. J Gerontol A Biol Sci Med Sci. 2018.
Knowler WC, Fowler SE, Hamman RF, et al. Long-term Effects of Metformin on Diabetes Prevention: Identification of Subgroups That Benefited Most in the Diabetes Prevention Program and Diabetes Prevention Program Outcomes Study. Diabetes Care. 2019.
Knowler WC, Diabetes Prevention Program Research Group, et al. Long-term Effects and Effect Heterogeneity of Lifestyle and Metformin Interventions on Type 2 Diabetes Incidence Over 21 Years in the US Diabetes Prevention Program Randomised Clinical Trial. Lancet Diabetes Endocrinol. 2025.
Goldberg RB, Orchard TJ, Crandall JP, et al. Effects of Long-term Metformin and Lifestyle Interventions on Cardiovascular Events in the Diabetes Prevention Program and Its Outcome Study. Circulation. 2022.
Aroda VR, Edelstein SL, Goldberg RB, et al. Long-term Metformin Use and Vitamin B12 Deficiency in the Diabetes Prevention Program Outcomes Study. J Clin Endocrinol Metab. 2016.
Witham MD, McDonald C, Wilson N, et al. Metformin and Physical Performance in Older People with Probable Sarcopenia and Physical Prefrailty or Frailty in England (MET-PREVENT): a Double-Blind, Randomised, Placebo-Controlled Trial. Lancet Healthy Longev. 2025.
Espinoza SE, Musi N, Wang CP, et al. Rationale and Study Design of a Randomized Clinical Trial of Metformin to Prevent Frailty in Older Adults With Prediabetes. J Gerontol A Biol Sci Med Sci. 2020.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.