GLP-1 and Functional Age: When Weight Loss Helps Longevity and When It Hurts
The public headline is weight loss. The longevity question is functional age: what happens to lean mass, strength, and cardiorespiratory capacity while body weight falls.
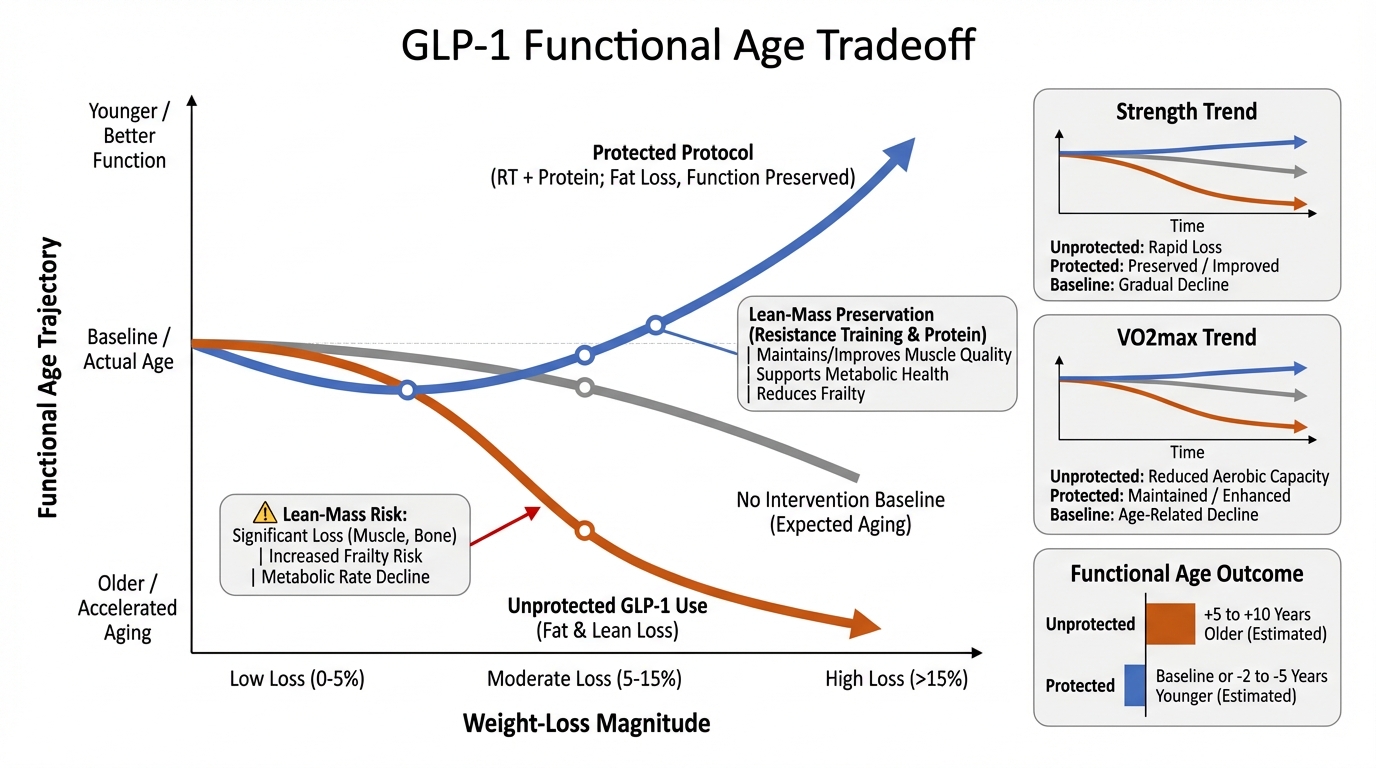
GLP-1 and dual incretin therapies can produce substantial metabolic improvement and meaningful weight reduction. But scale weight alone is a poor proxy for healthspan trajectory. If lean tissue and physical capacity decline while fat mass drops, the intervention can improve one risk domain while worsening another. For lifespan planning, the target is not lower weight by itself. The target is lower fat mass with preserved or improved function.
What Is Real Right Now
1) GLP-1 class therapies can improve cardiometabolic risk factors. Weight, glycemic control, and blood-pressure burden often move in the right direction in appropriately selected patients.
2) Lean mass loss is a real risk during pharmacologic weight loss. Reviews and analyses now quantify that not all lost mass is fat, especially without resistance training and protein strategy.
3) Clinical trial design is moving toward mitigation. Registries increasingly include protocols testing resistance training and nutrition support alongside GLP-1 treatment to preserve lean tissue.
What Is Overstated
Claim: “Any weight loss is longevity-positive.” Not always. Function can deteriorate if lean mass and strength fall materially.
Claim: “Body weight trend tells you enough.” It does not. Body composition and performance metrics are required to interpret true aging impact.
Claim: “Medication alone solves frailty risk.” False framing. Training, nutrition, sleep, and recovery are not optional in high-quality outcomes.
The Translation Layer: Functional Age vs Scale Weight
For longevity decisions, the most useful frame is a two-axis model: metabolic risk reduction on one axis and physical capacity retention on the other. The best outcome sits in the quadrant where both improve. This requires explicit co-interventions rather than passive hope that weight loss will preserve function automatically.
Strength and aerobic fitness are repeatedly linked to outcomes and resilience. A plan that lowers weight but deconditions the patient can be numerically successful while biologically fragile.
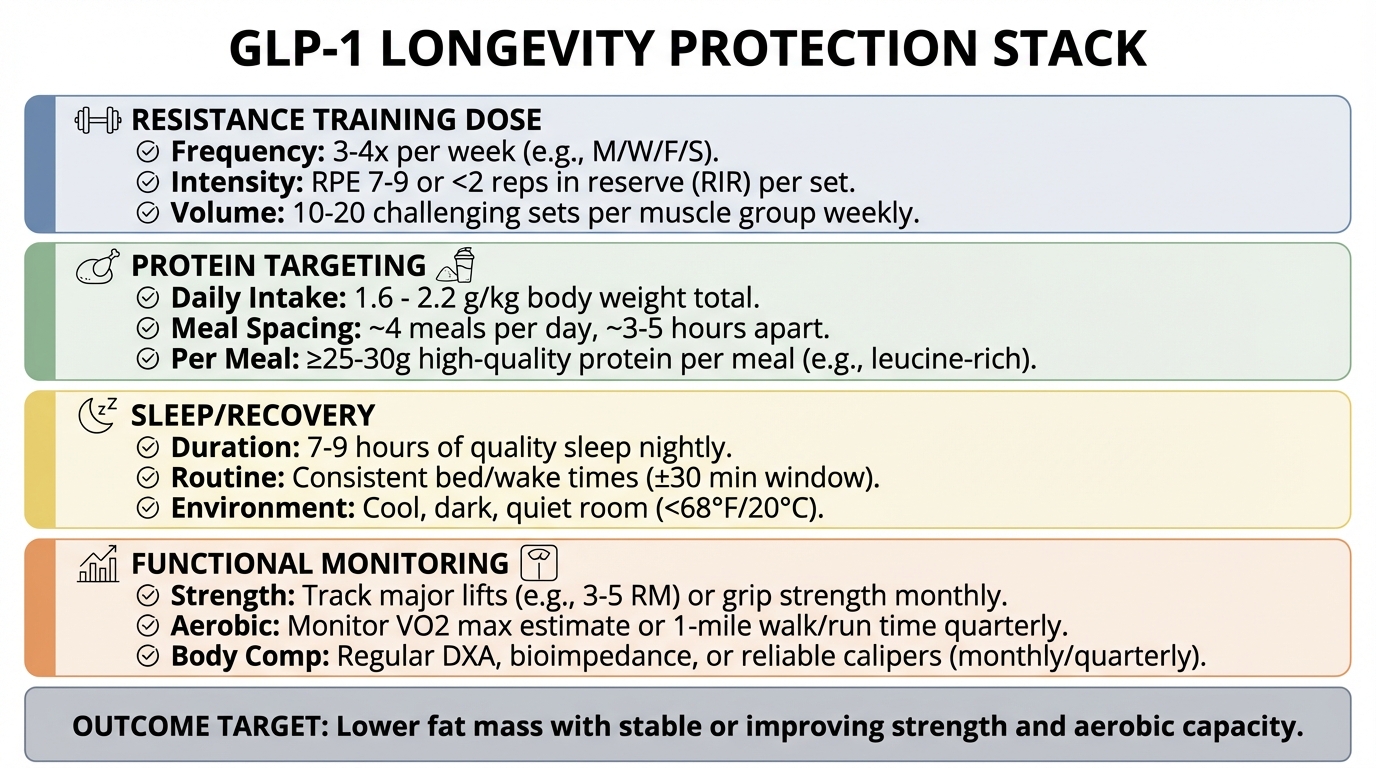
Intervention Stack That Protects Functional Age
1) Resistance training dose. Progressive loading 2-4 times per week with compound movements and performance tracking.
2) Protein strategy. Daily and per-meal targets to support retention of lean tissue during caloric deficit and appetite suppression.
3) Recovery controls. Sleep regularity and fatigue management to maintain training quality and adherence.
4) Monitoring loop. Follow waist trend, body composition proxy, strength markers, step/activity volume, and periodic labs.
Practical Monitoring Framework
Use weekly checks for adherence and activity, monthly checks for strength trend and circumference/body composition proxy, and quarterly checks for cardiometabolic markers. If strength and performance drop while weight falls, that is not a pass condition. It is a protocol adjustment trigger.
Key Takeaways
GLP-1 therapies can be longevity-positive, but only if functional decline is actively prevented.
Scale weight is not the endpoint for healthspan planning; function and composition are.
Resistance training, protein strategy, and recovery should be treated as core therapy, not add-ons.
The right outcome is fat loss with preserved or improved strength and aerobic capacity.
Source List
Hitaka, K., et al. (2026). Efficacy of GLP-1 analog peptides and dual incretin pathways (International Journal of Obesity).
Hierholzer, J., et al. (2026). Mitigating lean muscle loss in GLP-1 and dual incretin treatment (Nutrition, Metabolism & Cardiovascular Diseases).
Tinsley, G. M., et al. (2025). Preservation of lean soft tissue during GLP-1 induced weight loss (PubMed Central).
ClinicalTrials.gov (2026). Trials combining GLP-1 therapies with exercise/nutrition strategies.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.