Senolytics: From Mouse Lifespan Gains to Human Trials
The senolytic idea is simple enough to be seductive: some aged tissues accumulate cells that have stopped dividing but keep emitting inflammatory and tissue-disruptive signals, so remove those cells and function should improve. The biology is no longer fringe. The human claim is still unfinished.
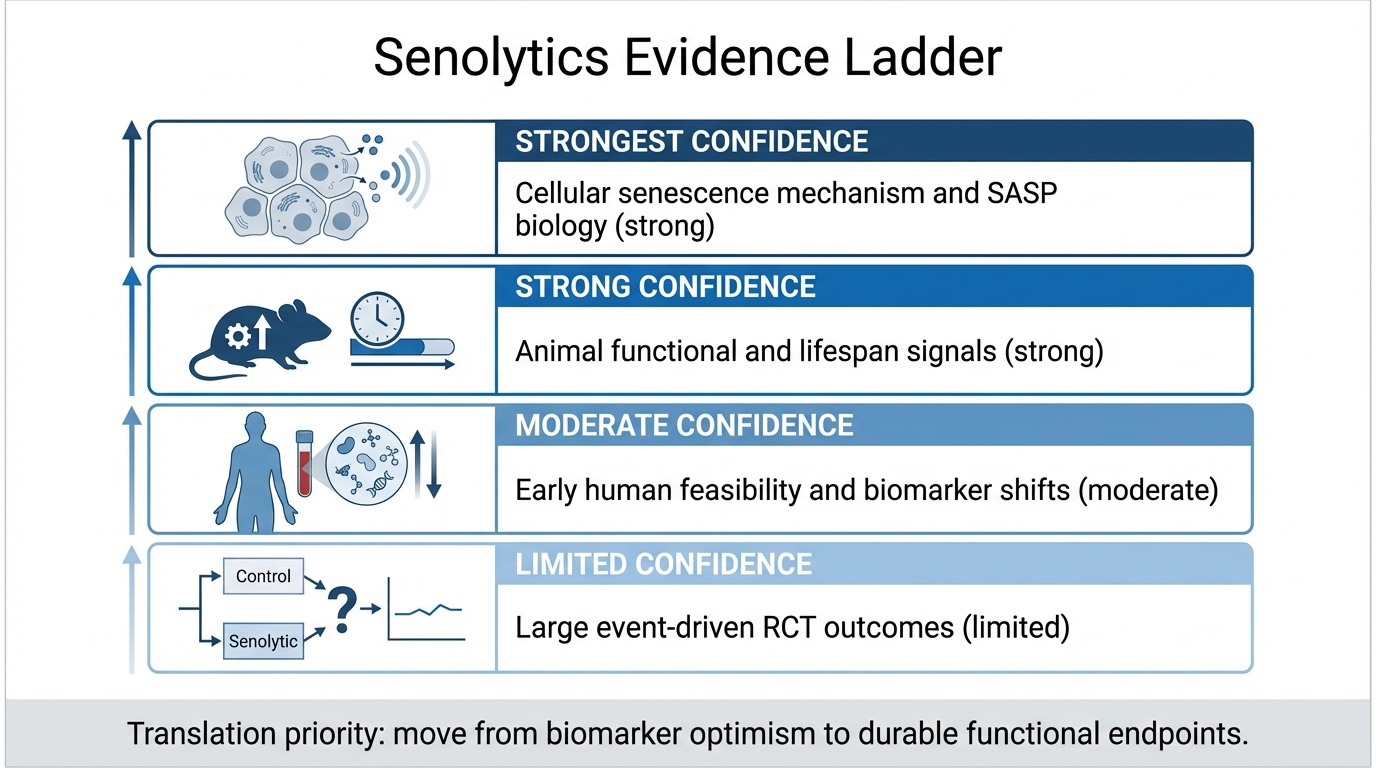
Established fact: senescent cells accumulate in many age-related disease contexts, and their senescence-associated secretory phenotype can damage neighboring tissue. Established fact: multiple mouse models show functional gains when senescent cells are genetically or pharmacologically reduced. Established fact: human studies of dasatinib plus quercetin have reached pilot and small randomized designs in serious disease cohorts. The inference is narrower than the excitement. Senolytics are plausible disease-modifying tools in selected indications, not validated broad anti-aging drugs.
Core thesis: senolytics have one of the strongest mechanistic stories in geroscience because they target burden rather than only signaling. The field has not yet shown that senescent-cell clearance produces durable, clinically meaningful benefit in large human trials. Until that happens, the correct status is serious translational hypothesis, not consumer longevity protocol.
Why The Mouse Evidence Mattered
The mouse evidence changed the field because it suggested that senescent cells were not merely markers of aging tissue. They could be causal contributors. Genetic clearance experiments and later pharmacologic work showed improvements across multiple systems, including adipose tissue, vascular function, physical performance, pulmonary fibrosis models, and metabolic dysfunction. These findings made senescence a therapeutic target rather than only a descriptive hallmark.
That matters because many aging mechanisms are difficult to intervene on cleanly. DNA damage, mitochondrial dysfunction, proteostatic decline, epigenetic drift, and immune aging all interact. Senolytics offered a more concrete intervention model: find cells using pro-survival pathways to resist apoptosis, disable those defenses intermittently, and let the damaged cells die. The logic is not that every senescent cell is bad. It is that persistent senescent-cell burden can become pathological when the tissue can no longer resolve it.
The mouse-to-human gap remains large. Laboratory strains, induced disease models, age windows, dosing schedules, and tissue turnover differ from real older adults with multimorbidity and polypharmacy. Mouse gains justify human trials. They do not set human effect sizes.
What Human Trials Have Actually Shown
The first meaningful human signals came from small studies using dasatinib plus quercetin, often abbreviated D+Q. In idiopathic pulmonary fibrosis, an open-label pilot reported feasibility and functional signals. A later small randomized pilot in IPF reported strong completion and adherence in twelve participants and treated the study mainly as feasibility and tolerability work. That is meaningful progress, but the sample was not designed to prove clinical efficacy.
In diabetic kidney disease, a preliminary D+Q trial reported reductions in senescent-cell markers in human adipose tissue and changes in inflammatory measures. The authors themselves cautioned against use outside clinical trials because the field was new, the treated human population remained small, and class-level risks were not yet known. That caution is not rhetorical. It is the correct translational boundary.
ClinicalTrials.gov records also show that these programs have been updated and extended over time, which indicates continued translational work rather than a completed proof base. The field is active. It is not settled.
The Critical Distinction: Target Engagement Versus Outcome Proof
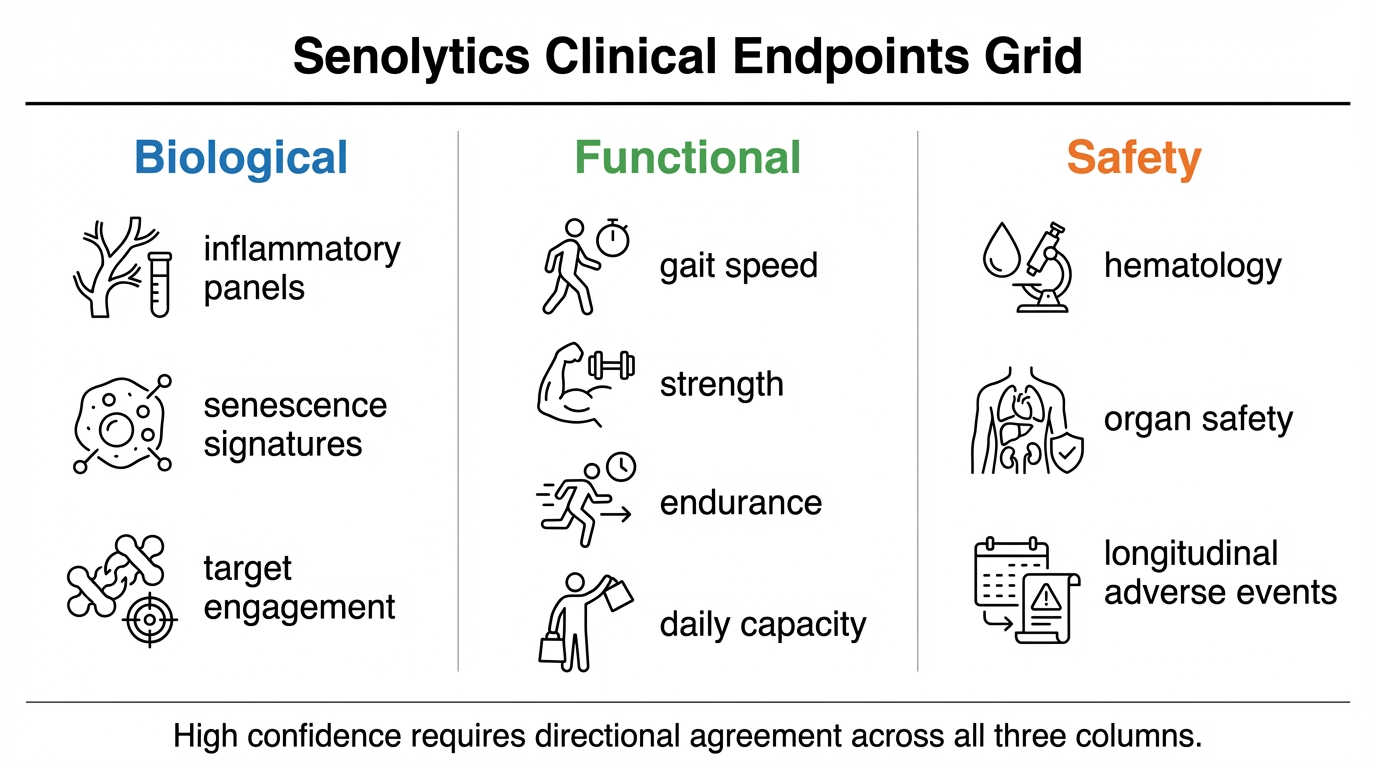
Target engagement asks whether the intervention changes the biology it claims to change. In senolytics, that means evidence of reduced senescent-cell burden, changed SASP output, or tissue-level movement consistent with clearance. Outcome proof asks whether patients actually do better in durable, clinically meaningful ways. Those are different standards.
Many early senolytic studies are more persuasive on target engagement than on outcomes. That is expected at this stage. A field should first show that the intervention reaches the target. The problem comes when target engagement gets marketed as if it already proves healthspan extension. A lower p16 signal, fewer senescence-associated markers, or a short-term functional change does not by itself establish reduced frailty, slower organ decline, fewer events, or longer healthy survival.
Why Safety Is Not A Side Issue
Senescence is not only damage. Transient senescence contributes to tumor suppression, wound repair, embryonic development, and tissue remodeling. A useful senolytic must therefore distinguish persistent harmful senescent cells from cells temporarily performing protective work. That is a hard pharmacologic problem.
Dasatinib is not a benign supplement. Navitoclax-class approaches raise platelet and hematologic concerns. Even flavonoid combinations cannot be assumed harmless when paired with targeted drugs or used in older adults with complex medication lists. The attractive intermittent dosing model may reduce exposure, but it does not remove the need for formal safety evidence.
The safety question also varies by tissue. Clearing senescent cells from fibrotic lung, osteoarthritic joint, adipose tissue, kidney-adjacent inflammatory compartments, or skin is not one clinical scenario. Each tissue has different regenerative capacity, different collateral-risk tolerance, and different ways to measure benefit. A serious trial program must be indication-specific.
Where The Field Looks Most Plausible
The strongest near-term use cases are not broad preventive longevity. They are disease settings where senescent-cell burden is plausibly part of pathology, where tissue access or biomarkers can show target engagement, and where functional endpoints are measurable. Idiopathic pulmonary fibrosis, diabetic kidney disease biology, osteoarthritis-related tissue degeneration, frailty phenotypes, and selected fibrotic or inflammatory conditions all fit parts of that logic. None automatically validates the others.
This is why the next decade of senolytics will probably look less like an anti-aging marketplace and more like a portfolio of disease-specific programs. Some may fail because the target is not causal enough. Some may fail because clearance is too blunt. Some may work only in enriched subgroups. That would not invalidate senescence biology. It would mean the biology has to be translated with clinical discipline.
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | Senescent cells and SASP signaling contribute to dysfunction across several age-related disease contexts. |
| Known | Mouse studies show that reducing senescent-cell burden can improve function and disease phenotypes in multiple systems. |
| Known | Human D+Q studies have shown feasibility, tolerability signals, and preliminary biological target engagement in small cohorts. |
| Inferred | Senolytics are most likely to prove useful where persistent senescent-cell burden is a driver of tissue pathology rather than a bystander marker. |
| Unknown | Whether any senolytic regimen can produce replicated, durable human benefit on organ function, disability, event rates, or survival with acceptable long-term safety. |
What Would Change The Evidence Grade
- Large randomized trials. The field needs studies powered for functional or disease outcomes, not only biomarker shifts.
- Tissue-level target engagement. Circulating inflammatory movement is useful, but it cannot replace evidence in the target tissue.
- Durability after intermittent dosing. If the intervention claims hit-and-run repair, benefit should persist beyond immediate exposure.
- Replication across independent teams. A mature field cannot depend on one compound pair, one lab network, or one disease model.
- Clear exclusion of consumer overreach. Trials in serious disease do not justify unsupervised preventive dosing in healthy adults.
The Practical Reading For 2026
Senolytics deserve attention because the causal hypothesis is unusually direct for aging biology. They also deserve restraint because the human endpoint layer remains underbuilt. The correct question is not whether senolytics are real. They are real enough to test seriously. The correct question is which tissues, which patients, which regimens, and which outcomes can survive a clinical standard.
For LifeMeter readers, the disciplined position is strict. Treat senolytics as an advanced translational program, not as a proven longevity intervention. Give high weight to trials that show tissue target engagement plus functional benefit. Give low weight to claims that extrapolate from mouse lifespan gains or short biomarker movement directly to human anti-aging use.
Further Reading Inside The Site
This article connects directly to Senomorphics vs Senolytics, Hallmarks of Aging Revisited, and Is Aging a Disease or an Adaptive Program?. Together they separate senescence biology, intervention style, and clinical evidence grade.
Source List
Nambiar AM, et al. Senolytics dasatinib and quercetin in idiopathic pulmonary fibrosis: randomized pilot trial. EBioMedicine. 2023.
Justice JN, et al. Senolytics in idiopathic pulmonary fibrosis: first-in-human open-label pilot study. EBioMedicine. 2019.
Hickson LJ, et al. Senolytics decrease senescent cells in humans: preliminary diabetic kidney disease trial report. EBioMedicine. 2019.
Zhang L, Pitcher LE, Prahalad V, Niedernhofer LJ, Robbins PD. Targeting cellular senescence with senotherapeutics: senolytics and senomorphics. FEBS Journal. 2023.
ClinicalTrials.gov. Senescence in Chronic Kidney Disease, NCT02848131. Record updated June 4, 2025. Accessed April 22, 2026.
Bian X, et al. Senolytics, dasatinib plus quercetin, reduce kidney inflammation and senescent-cell abundance in murine diabetic kidney disease. EBioMedicine. 2026.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.