Senomorphics vs Senolytics: Slowing vs Removing Damage
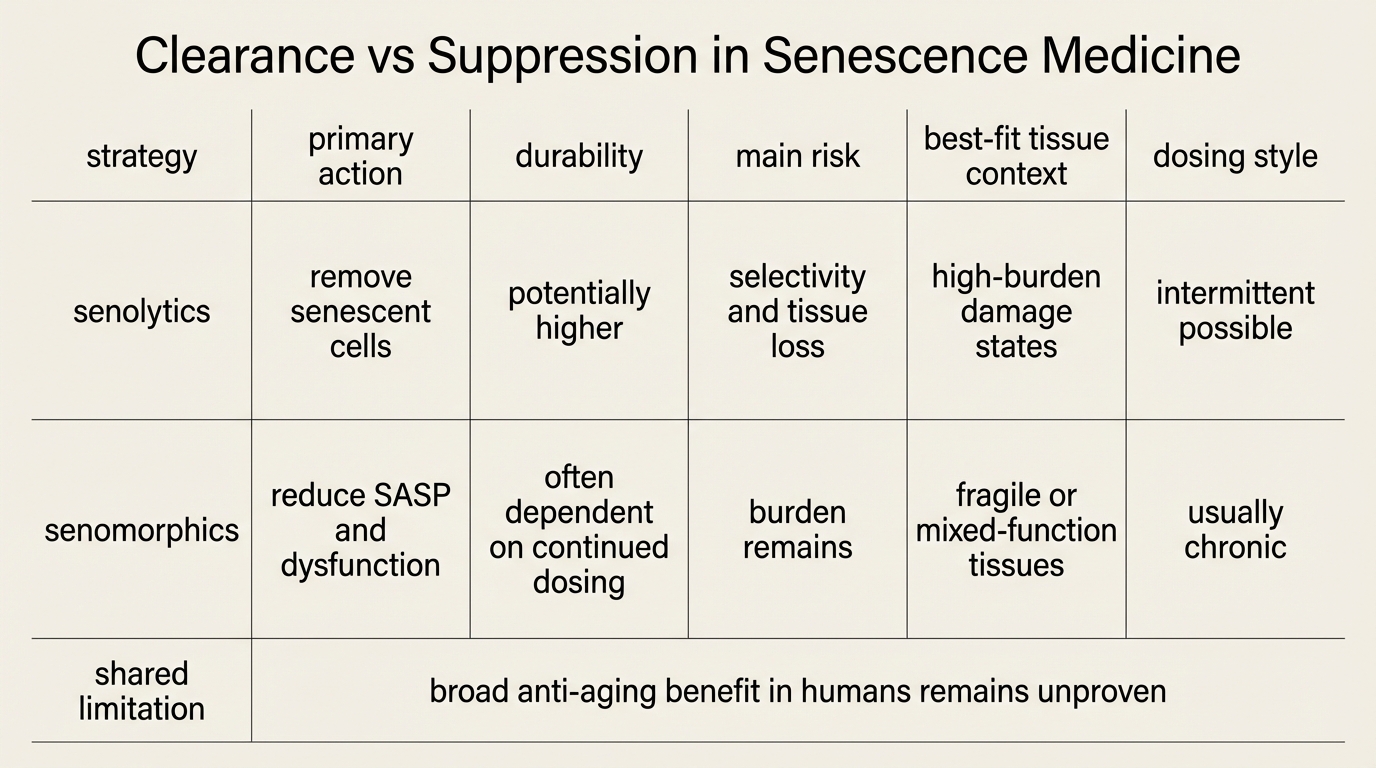
Senescence medicine is now split between two intervention logics. Senolytics try to kill senescent cells. Senomorphics try to keep those cells alive while suppressing the inflammatory and matrix-degrading signals that make them dangerous. That distinction is not semantic. It defines the real tradeoff between mechanistic force and biological restraint.
Established fact: persistent senescent cells accumulate with age and contribute to tissue dysfunction through growth arrest, altered metabolism, and the senescence-associated secretory phenotype, or SASP. Established fact: animal models show that removing part of that burden can improve function across several organs. Established fact: senescence itself is not purely pathological because transient senescence helps with tumor suppression, wound repair, and developmental patterning. The practical question is therefore narrower than many headlines imply. It is not whether senescence matters. It is whether a given tissue is better served by suppression, selective clearance, or no direct senescence intervention at all.
Core thesis: senolytics remain the more aggressive and potentially more transformative strategy because they reduce senescent-cell burden directly. Senomorphics remain the more conservative and often more plausible near-term strategy because they try to reduce harmful signaling without forcing cell death in tissues where senescence may still have protective roles. The human evidence does not yet justify broad anti-aging use for either class.
What Each Strategy Actually Does
Senolytics aim at selective elimination. The usual logic is that senescent cells survive by leaning on senescent-cell anti-apoptotic pathways, so the drug should disable those survival programs and let the damaged cell die. Dasatinib plus quercetin, navitoclax-derived approaches, and several newer targeted platforms follow that basic structure. When the target is real and selectivity is adequate, senolytics reduce the burden rather than merely hiding the phenotype.
Senomorphics aim at modulation. Instead of clearing the cell, they try to reduce the SASP, dampen inflammatory signaling, or shift the cell into a less harmful state. Rapamycin-pathway interventions, JAK-pathway modulation, metformin-adjacent signaling effects, and other anti-inflammatory or nutrient-sensing interventions are often discussed in this frame. The appeal is obvious: if senescent cells are heterogeneous and some remain useful or at least less dangerous than others, a modulation strategy may preserve beneficial functions while lowering collateral damage.
The biological divide matters because the mechanisms imply different failure modes. A weak senolytic leaves the bad cells behind. A strong but insufficiently selective senolytic risks harming non-senescent cells or destabilizing tissue repair. A senomorphic can lower harmful signaling while leaving the underlying burden in place, which may require chronic dosing and may permit re-escalation once treatment stops.
Why Senolytics Still Command More Attention
The case for senolytics is stronger at the mechanistic level because clearance is a cleaner intervention than suppression. If persistent senescent cells are causally harmful, then physically reducing that pool should have larger downstream effects than only turning down one part of their secretory output. This is why mouse data generated so much enthusiasm. Across several models, reducing senescent-cell burden improved function in bone, adipose tissue, lung, vasculature, and other systems. The signal is not universal, but it is broad enough to support serious translational work.
Early human work also exists, which matters even though it remains small. The first-in-human idiopathic pulmonary fibrosis pilot using dasatinib and quercetin reported feasibility and functional signal, not definitive proof. Later translational reviews from the Kirkland and Niedernhofer groups framed the field more carefully: promising pilots, incomplete endpoint depth, and a pressing need for better biomarkers, larger trials, and clearer target engagement. That is the right reading. Senolytics are clinically interesting because they may change burden rather than just symptoms. They are not clinically established because the human evidence base is still thin and heterogeneous.
Another reason senolytics attract interest is dosing logic. If clearance works, it may not need continuous exposure. Intermittent dosing is one of the field's most attractive ideas because it suggests a way to limit chronic toxicity. That advantage is still partly inferred from preclinical work and early trial design rather than from a mature clinical literature, but it is a real strategic difference from drugs that must suppress signaling indefinitely.
Why Senomorphics May Fit More Realistic Near-Term Use Cases
Senomorphics are often framed as the weaker option. That is too simple. In some tissues they may be the better first move precisely because senescence is not always a disposable state. Transient senescence contributes to wound healing and can restrain malignant transformation. Even persistent senescent populations are heterogeneous across tissues and disease states. A blunt clearance program may therefore remove cells that are harmful in one context but compensatory in another.
This is where modulation becomes attractive. If the dominant damage comes from inflammatory secretions, extracellular-matrix remodeling, or paracrine dysfunction, then lowering those outputs may improve the tissue environment while avoiding the collateral cost of cell loss. The price is usually chronicity. Senomorphics often look more like long-duration disease management than hit-and-run repair. That can still be rational if the tissue is fragile, the burden is diffuse, or the clearance tools remain too toxic or too imprecise.
There is a second practical advantage. Many agents described as senomorphic sit closer to existing clinical pharmacology than true senolytics do. That does not make them validated aging drugs. It does make them easier to test inside disease-specific populations, particularly where inflammatory tone, frailty progression, or fibrosis biology already provide tractable endpoints. The likely near-term result is not a clean winner between the two classes. It is a split market of indications, tissues, and risk tolerances.
Where The Hype Usually Goes Wrong
The most common mistake is to treat the entire senescence field as though it already had one unified therapeutic answer. It does not. Senescence is heterogeneous. The SASP is heterogeneous. The tissue consequences are heterogeneous. A claim that “senolytics cure aging” or “senomorphics are safer therefore better” collapses too many biological variables into one slogan.
The second mistake is to assume that biomarker movement proves healthspan translation. Reduced inflammatory markers, lower expression of selected senescence genes, or a shift in a tissue biopsy can all be useful. None of them alone demonstrate durable benefit in physical function, organ performance, disability, or survival. The more the field moves toward consumer-facing longevity narratives, the more this distinction matters.
The third mistake is to ignore replacement biology. Clearing senescent cells can be useful only if tissue function stabilizes or improves afterward. In older organisms with limited regenerative capacity, cell removal is not automatically a free gain. Modulation has the opposite problem. Suppressing harm without changing burden may leave the tissue in a chronic holding pattern that looks better on paper than it performs over time. Both strategies therefore require organ-specific endpoint discipline rather than one cross-aging marketing story.
What A Serious Clinical Standard Would Look Like
- Tissue specificity. Trials should state clearly which senescent population is being targeted and why that population is believed to drive pathology in that organ.
- Target engagement. Programs need better evidence that treatment actually changes senescent-cell burden or SASP output in human tissue, not only in circulation.
- Functional endpoints. Movement in fibrosis burden, frailty, gait, exercise tolerance, pain, organ reserve, or other clinically meaningful outcomes matters more than biomarker motion alone.
- Durability accounting. If an intervention works only during continuous dosing, that should be stated plainly rather than treated as a minor implementation detail.
- Safety by tissue context. The tolerance for cell elimination in fibrotic lung, osteoarthritic joint, skin aging, and systemic preventive use is not the same and should not be regulated or narrated as if it were.
This is why the field remains promising rather than settled. Senolytics have the cleaner causal ambition. Senomorphics have the cleaner near-term safety logic. Neither class has yet crossed the line into broad human anti-aging validation.
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | Persistent senescent cells and their secretory phenotype contribute to tissue dysfunction across multiple age-related conditions. |
| Known | Senolytics and senomorphics are biologically distinct strategies: one aims to eliminate senescent cells, the other aims to suppress their harmful behavior. |
| Known | Early senolytic human studies show feasibility and directional signal, but they do not yet establish broad healthspan benefit or long-term safety. |
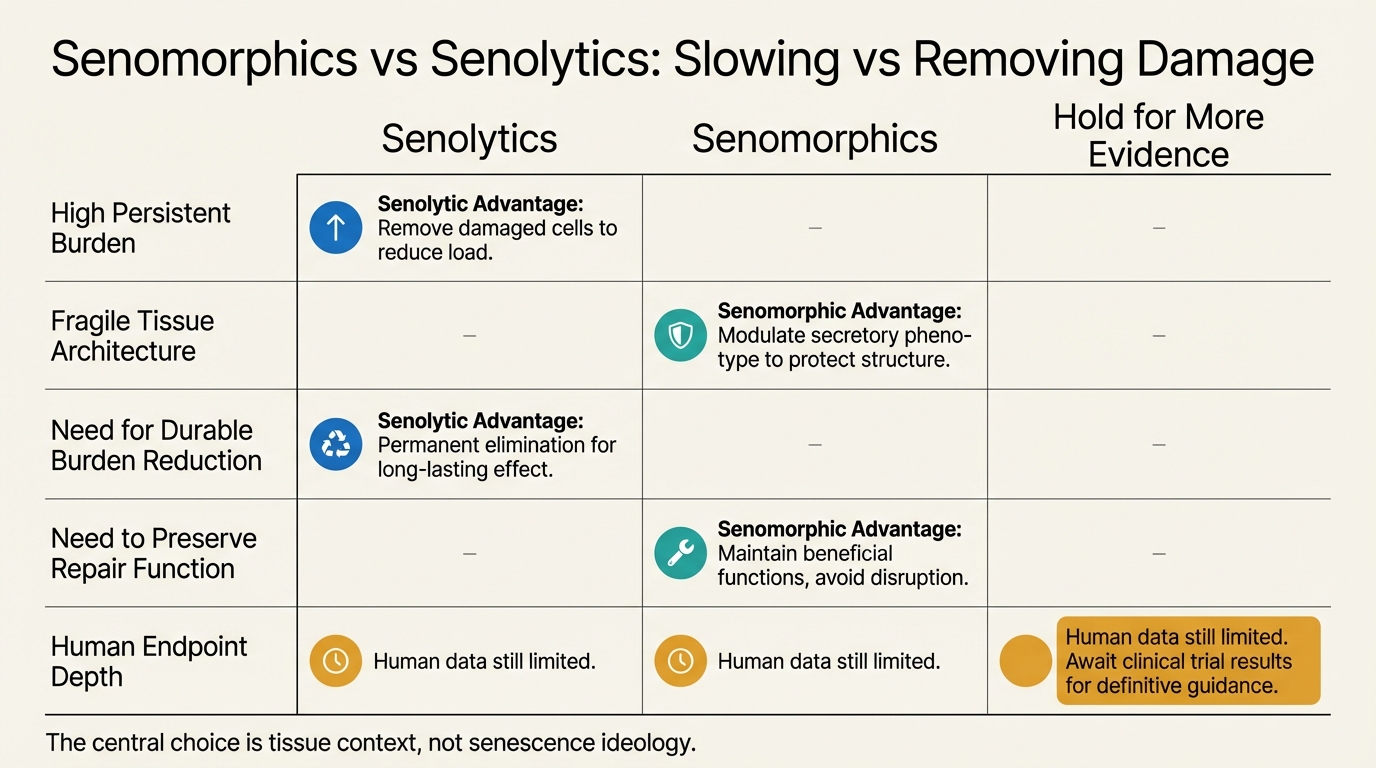
| Inferred | Senolytics are more likely to matter where accumulated burden itself is the dominant problem, while senomorphics may fit fragile tissues or indications where preserving structure matters more than aggressive clearance. |
| Unknown | Which organs, dosing schedules, and patient groups will prove that direct senescence intervention changes meaningful human outcomes better than high-quality standard care. |
The Practical Reading For 2026
The disciplined position is not to pick a philosophical side. It is to ask what pathology is being targeted, whether burden reduction or phenotype suppression is the more coherent mechanism in that setting, and whether the human evidence has advanced beyond pilot-stage plausibility. Today that usually yields a restrained answer. Senolytics still hold the more ambitious upside. Senomorphics still look easier to fit into near-term clinical experimentation. The strongest claim either class can support is still conditional and disease-specific.
For LifeMeter readers, the useful conclusion is strict. If an intervention cannot state whether it is removing senescent cells or only damping their output, it is not ready for serious translational confidence. If it can state the mechanism but cannot show durable human benefit in the relevant tissue, it remains an active hypothesis rather than a validated longevity tool.
Further Reading Inside The Site
This article connects directly to Senolytics Moving into Clinical Translation, Metformin as a Longevity Drug: Evidence vs Assumption, and Is Aging a Disease or an Adaptive Program?. Together they show how mechanistic plausibility, intervention style, and endpoint discipline change the real strength of a longevity claim.
Source List
Zhang L, Pitcher LE, Prahalad V, Niedernhofer LJ, Robbins PD. Targeting cellular senescence with senotherapeutics: senolytics and senomorphics. FEBS Journal. 2023.
Saliev T, Singh PB. Targeting Senescence: A Review of Senolytics and Senomorphics in Anti-Aging Interventions. Biomolecules. 2025.
Justice JN, Nambiar AM, Tchkonia T, et al. Senolytics in idiopathic pulmonary fibrosis: Results from a first-in-human, open-label, pilot study. EBioMedicine. 2019.
Niedernhofer LJ, Robbins PD. Strategies for late phase preclinical and early clinical trials of senolytics. Mechanisms of Ageing and Development. 2021.
Gorgoulis V, Adams PD, Alimonti A, et al. Cellular Senescence: Defining a Path Forward. Cell. 2021.
Wyles SP, Carruthers JD, Dashti P, et al. Cellular Senescence in Human Skin Aging: Leveraging Senotherapeutics. Gerontology. 2024.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.