One Injection vs Lifetime Statins: What the CRISPR Cholesterol Trial Actually Shows
A one-time CRISPR treatment that lowers LDL cholesterol sounds like the end of daily statins. That is the headline version. The evidence is more nuanced and more useful.
The first-in-human CTX310 trial targeting ANGPTL3 reported that a single infusion reduced LDL by about 50% and triglycerides by about 55% at the highest tested doses in a small Phase 1 study. Those are attention-grabbing numbers, but they are early numbers from a short follow-up window in a trial designed primarily for safety.
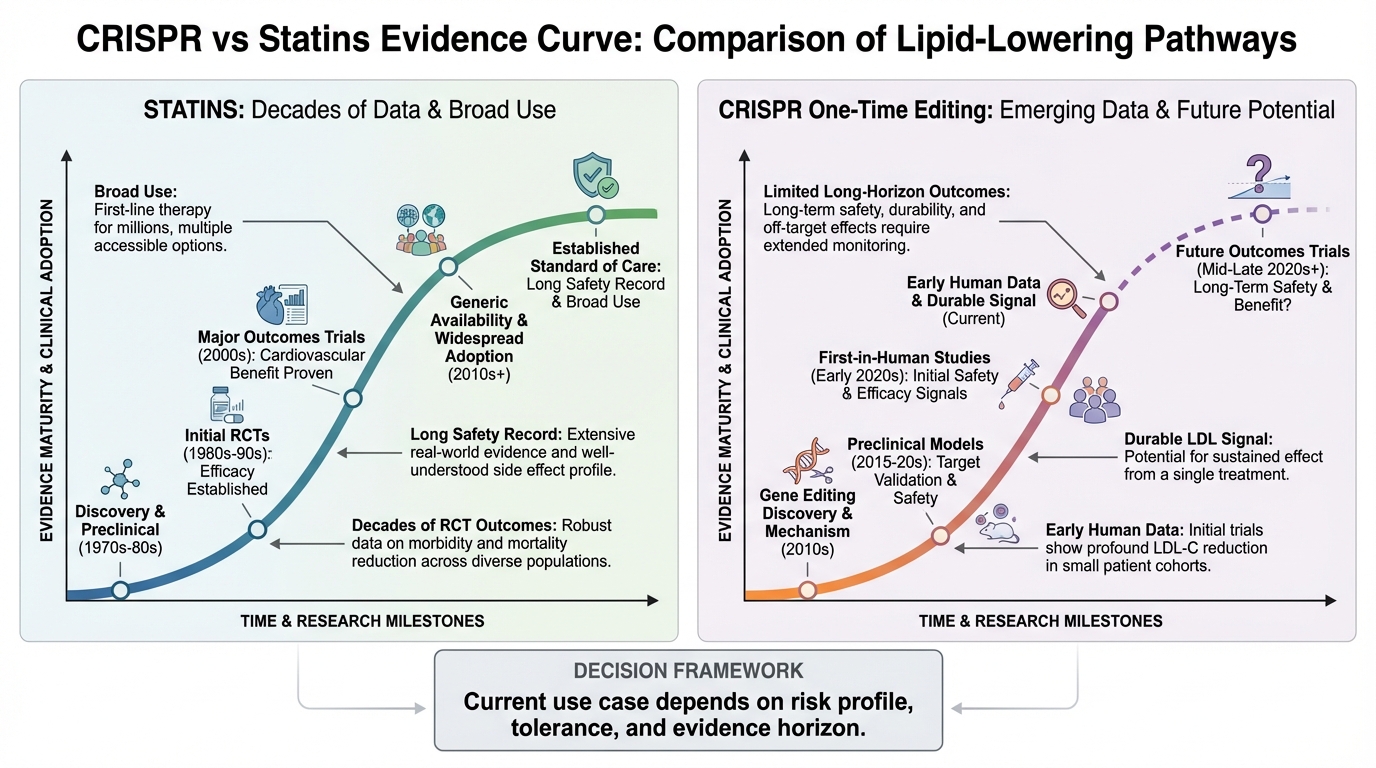
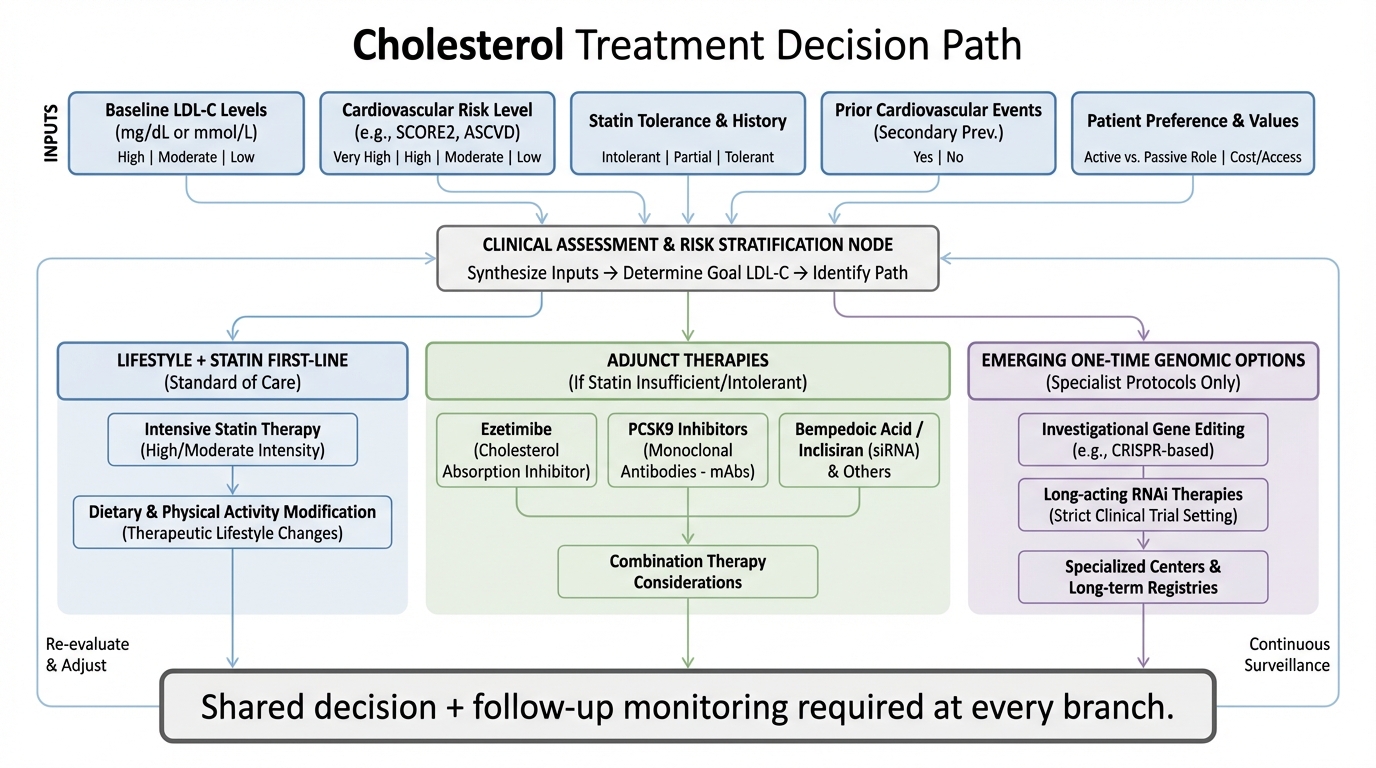
The right framing is not CRISPR versus statins as if one winner is already decided. The right framing is timelines and use cases. Statins have decades of outcomes data, broad cost access, and guideline integration. CRISPR lipid editing has strong early biological signal, major convenience potential, and a realistic chance to help patients who struggle with adherence or remain uncontrolled despite maximally tolerated therapy.
What the CTX310 Trial Actually Showed
The CTX310 Phase 1 study tested a one-time CRISPR-Cas9 infusion designed to knock down ANGPTL3 expression in the liver. At higher doses, LDL and triglycerides dropped substantially, with effects seen within about two weeks and sustained through the analysis window of at least 60 days for participants included in that cut. The enrolled population was small, with 15 adults across dose cohorts, and included patients with severe lipid disorders not adequately controlled on current treatment.
Safety findings were encouraging but early. Reported events included mild infusion reactions in some participants and a temporary liver-enzyme increase in one participant with pre-existing elevation, which resolved. Regulators generally require long-term monitoring for CRISPR-based interventions because gene editing is intended to be durable.
What Statins Still Do Better Right Now
Statins are not exciting, but they are proven at scale. Current cholesterol management guidance continues to rely on statin intensity because LDL reduction from statins has consistent links to lower cardiovascular event risk. High-intensity statins generally target at least 50% LDL reduction, while moderate-intensity therapy typically targets 30% to 49%.
In other words, the magnitude seen in high-dose CTX310 looks competitive on LDL lowering. The difference is certainty. Statins have extensive longitudinal data and real-world implementation frameworks. CTX310 does not have that yet.
Where One-Time Gene Editing Could Win
The strongest near-term value proposition is adherence and residual risk in hard-to-control patients. Nonadherence to chronic lipid medication is a persistent problem. One-and-done biology could change that equation if safety and durability continue to hold.
There is another strategic advantage in the ANGPTL3 target itself. Human loss-of-function evidence suggests lower LDL and triglycerides with lower atherosclerotic risk, strengthening biological plausibility for therapeutic inhibition.
What Is Overstated in Current Coverage
Overstatement 1: "Statins are finished." They are not. Statins remain foundational because outcomes evidence is deep and broad.
Overstatement 2: "The trial proves permanent cure." It does not. The trial shows early durable signal over weeks to months, not lifetime cure.
Overstatement 3: "Any patient with high LDL should switch." Not supported. Early-phase participants were selected high-need populations.
What Comes Next in the Evidence Timeline
The next checkpoints are larger Phase 2 validation, longer durability data, and outcome-oriented evidence showing that biochemical improvements translate into fewer clinical events over time. This is normal sequencing, but stakes are higher with permanent editing interventions.
Speculation, clearly labeled: The most plausible medium-term scenario is hybrid care, not replacement care. Statins and conventional therapies continue to dominate broad population management, while gene-editing approaches become high-value options for selected high-risk groups and then expand as long-term safety and economics improve.
How to Read the "One Injection" Narrative
Ask four questions: was the endpoint lipid change or hard outcomes, how long was follow-up, how large/diverse was the treated population, and what safety signals plus monitoring commitments were reported. If those answers are narrow, treat the news as high-quality early signal, not clinical finality.
Key Takeaways
The CTX310 Phase 1 result is a serious milestone, with around 50% LDL and 55% triglyceride reductions at high doses in early human data.
It is still early-stage evidence with small sample size and short follow-up, so it does not replace statin-first care.
The strongest near-term use case is likely high-risk, hard-to-control patients where adherence and residual risk remain major problems.
The long-term winner is likely a layered model where proven low-cost therapies and advanced one-time interventions coexist.
Source List
American Heart Association (2025). First-in-human trial of CRISPR gene-editing therapy safely lowered cholesterol and triglycerides.
Cleveland Clinic (2025). First-in-human trial of CRISPR gene-editing therapy shown to safely lower cholesterol and triglycerides.
American College of Cardiology (2025). First-in-human trial suggests CRISPR-Cas9 therapy targeting ANGPTL3 is safe and reduces LDL and triglycerides.
AHA/ACC (2018). 2018 Guideline on the management of blood cholesterol.
CRISPR Therapeutics (2025). Additional Phase 1 data update for CTX310 targeting ANGPTL3.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.