The Primary-Care Alzheimer's Pivot: What Blood Biomarkers Can and Cannot Do
Primary care now has a biomarker-era triage tool for cognitive decline. That does not create diagnosis certainty, and it does not remove the need for staged clinical reasoning.
The last five months changed the Alzheimer pathway more than most clinics have operationally absorbed. Blood-based amyloid and tau markers moved from specialist-centric discussion into a front-door decision point for routine practice. This is a meaningful expansion of access, but it is not a substitute for cognitive assessment, medication review, depression screening, sleep evaluation, neurologic examination, and structured follow-up.
The practical question is no longer whether biomarkers matter. The practical question is where they belong in sequence. Poor sequence creates over-referral, false reassurance, and delayed diagnosis for people who needed escalation. Good sequence improves signal detection while preserving specialist capacity for higher-likelihood cases.
Core thesis: blood biomarkers should be treated as triage multipliers inside a layered pathway, not as standalone diagnostic endpoints.
What Changed in the Last Five Months
Regulatory and commercial momentum accelerated blood biomarker adoption discussions in 2025 and early 2026. That acceleration shifted expectations among patients and clinicians. Patients increasingly ask for a blood test as a first move. Clinicians increasingly need an operational script for pre-test counseling, post-test interpretation, and referral thresholds.
The risk is process drift. If implementation is test-first without context-first, positive predictive value falls in low-prevalence settings. If implementation is context-first plus risk stratification plus test interpretation, utility rises and unnecessary specialist traffic falls.
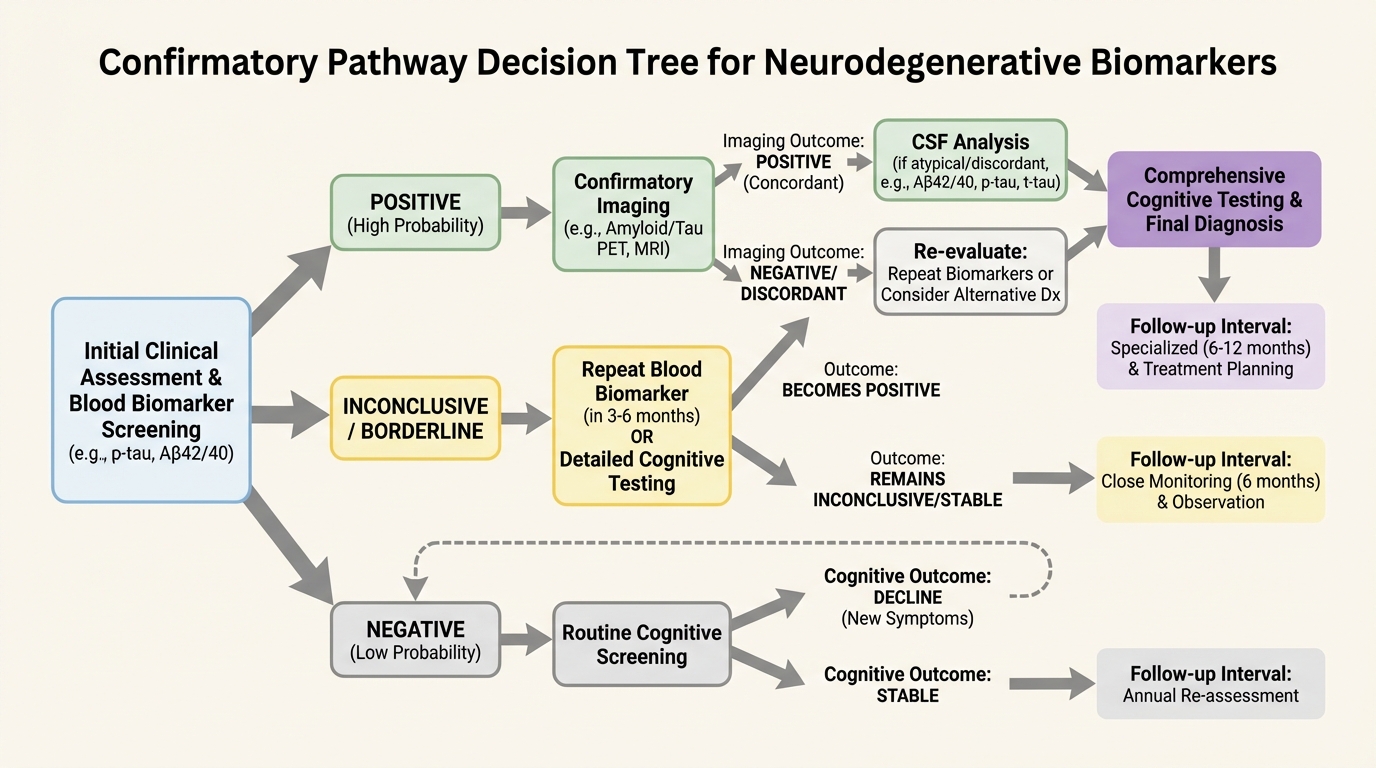
What Blood Biomarkers Can Do Reliably
- Increase confidence in whom to escalate earlier for confirmatory workup.
- Reduce delay for high-risk patients with converging cognitive and biomarker signals.
- Support consistent longitudinal tracking in clinics with disciplined follow-up protocols.
- Improve communication around risk staging when paired with function and cognition trends.
What They Cannot Do Reliably
- Replace differential diagnosis when depression, sleep disorders, vascular disease, medications, or delirium risk are present.
- Guarantee disease progression speed for a specific person.
- Resolve treatment eligibility without full clinical context and payer pathway requirements.
- Deliver low-error performance when deployed indiscriminately in very low pretest probability populations.

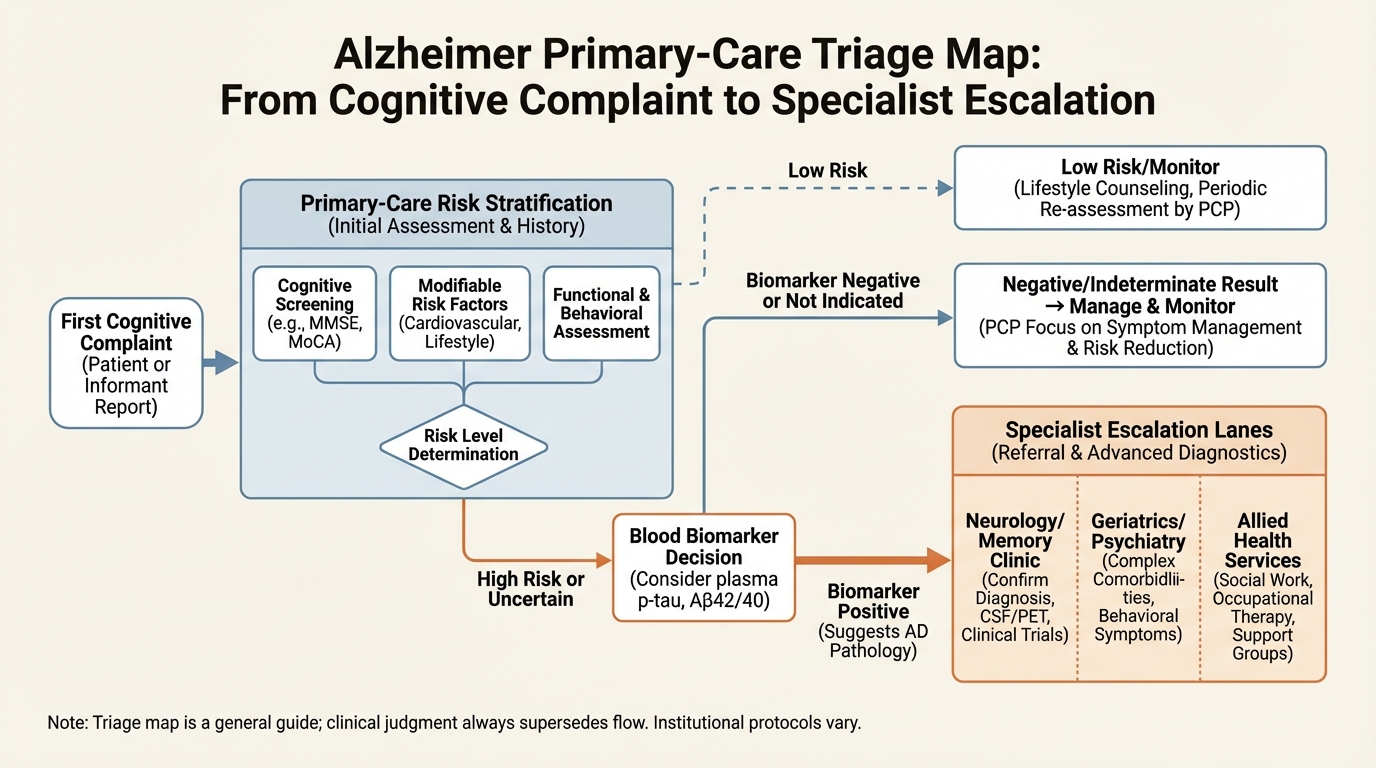
A Practical Referral Architecture
Primary care teams need explicit decision thresholds. A robust architecture uses three lanes. Lane one: low-risk presentation with no progressive signal, where monitoring and reversible-factor correction dominate. Lane two: intermediate uncertainty, where biomarkers can inform whether to escalate rapidly or continue structured observation. Lane three: high-risk progression, where specialist referral and confirmatory testing proceed regardless of biomarker ambiguity.
This lane model prevents both extremes that currently cause harm: overconfidence in a single laboratory result, and delayed escalation despite clear longitudinal decline.
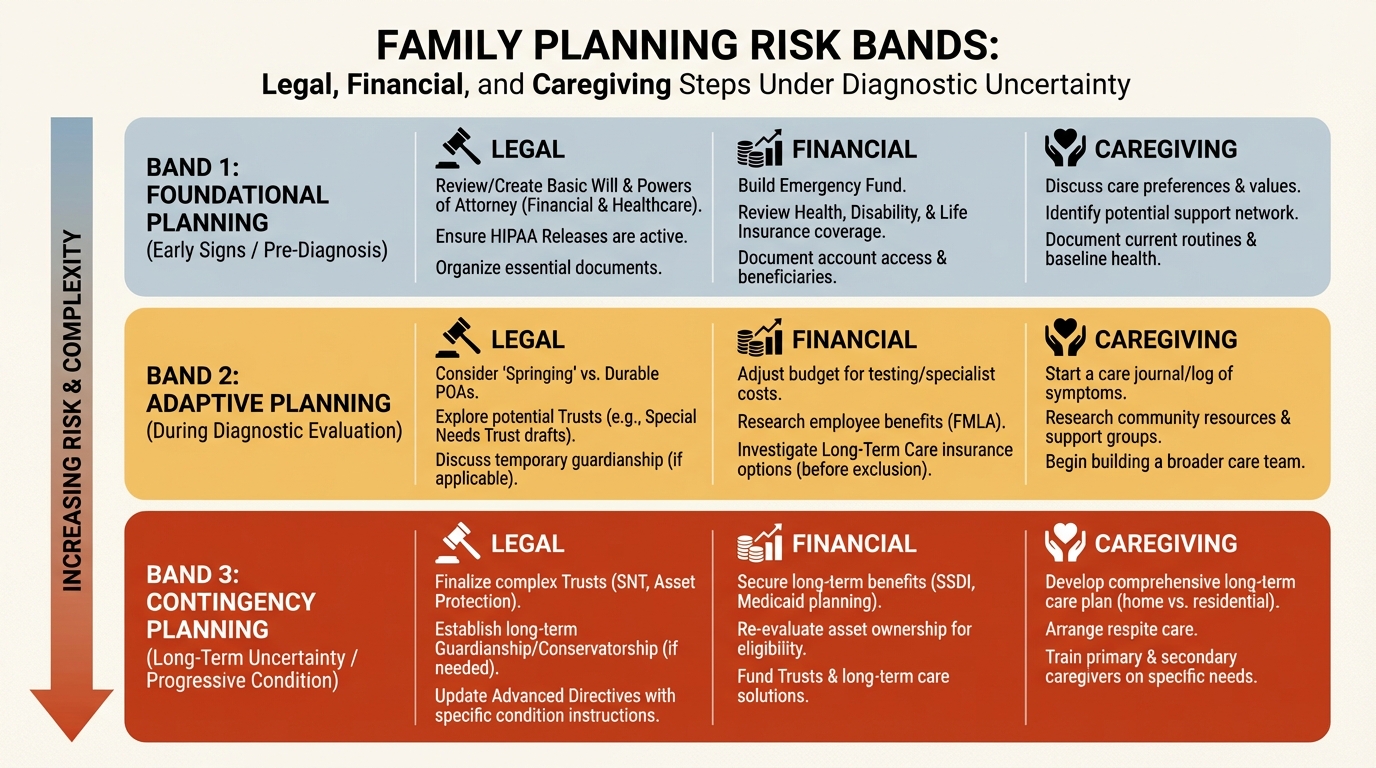
Household Planning Under Diagnostic Uncertainty
Families do not only need diagnosis labels. They need planning intervals, trigger points, and reversible actions that reduce downstream crisis probability. The most valuable immediate actions are legal and financial readiness, driving safety checkpoints, medication simplification, fall risk reduction, and care-network load sharing before emergency events force decisions.
The policy-level promise of earlier detection becomes real only when households get operational instructions that convert uncertainty into staged action.
Operational Bottom Line
The Alzheimer blood-test era is clinically significant, but its value depends on pathway design. Clinics that implement context-first triage, explicit escalation thresholds, and recurring reassessment will benefit. Clinics that implement test-first shortcuts will create noise, anxiety, and referral congestion.
Source List
Roche announcement on FDA clearance and intended primary-care use: Roche investor update.
U.S. NIH Alzheimer biomarker context and trial ecosystem: NIA biomarker overview.
Alzheimer's Association clinical guidance background: Alzheimer's Association biomarkers.
FDA device and diagnostics framework context: FDA IVD overview.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.