The 2026 Dyslipidemia Rewrite: Lp(a), ApoB, and 30-Year Risk in Preventive Longevity
The 2026 dyslipidemia update shifts prevention from short-term event counting to cumulative exposure management. That is a major change for longevity-oriented care.
Recent guideline updates emphasize risk architecture, not single-marker obsession. LDL-C remains important, but apoB and Lp(a) now play a larger role in treatment intensity decisions and residual-risk interpretation. This aligns prevention with first-principles vascular biology: cumulative atherogenic exposure is the real substrate of long-horizon events.
Core thesis: modern lipid prevention requires an integrated marker stack with risk equations and reclassification tools, not LDL-only heuristics.
What Changed in Practice
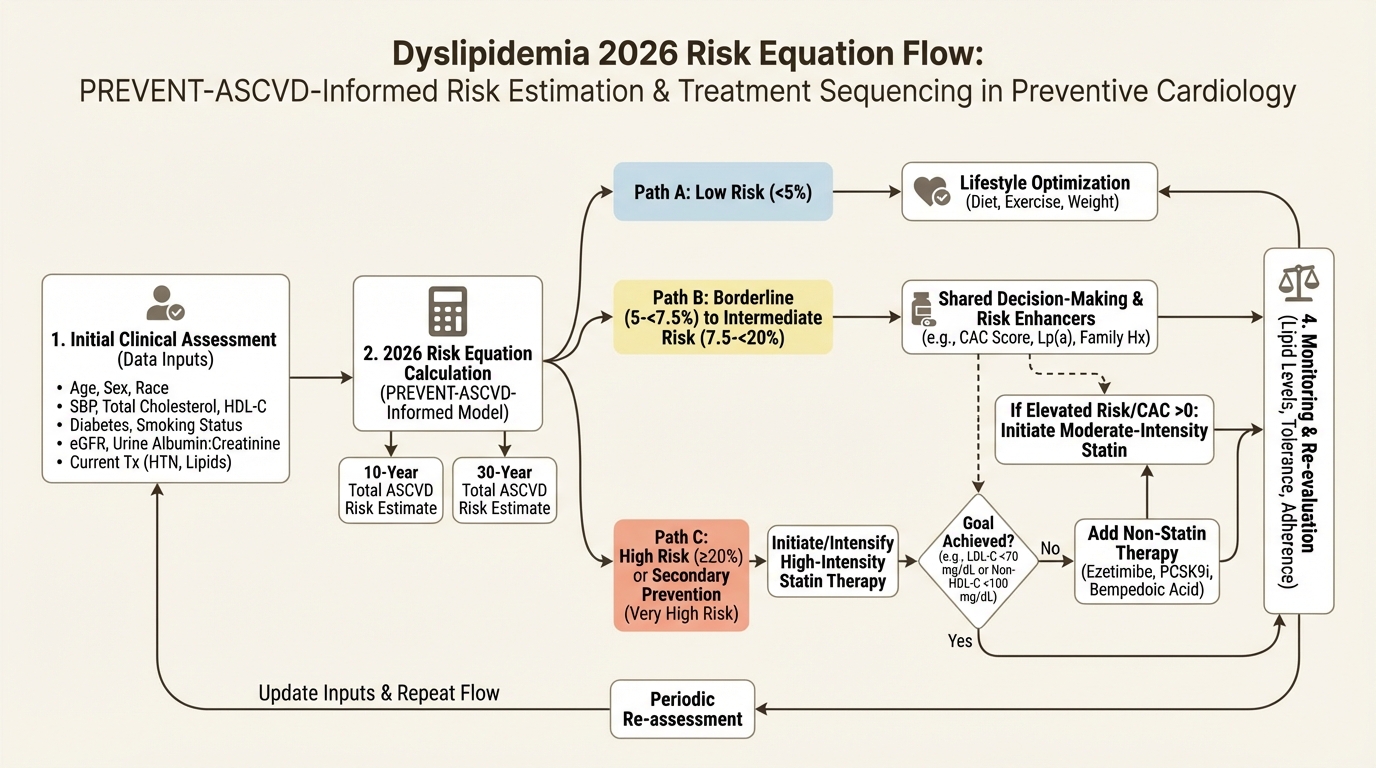
- Broader use of PREVENT-ASCVD frameworks for more granular risk estimation.
- Higher relevance of apoB and non-HDL cholesterol in discordant profiles.
- Lp(a) testing as a structural-risk identifier rather than a niche add-on.
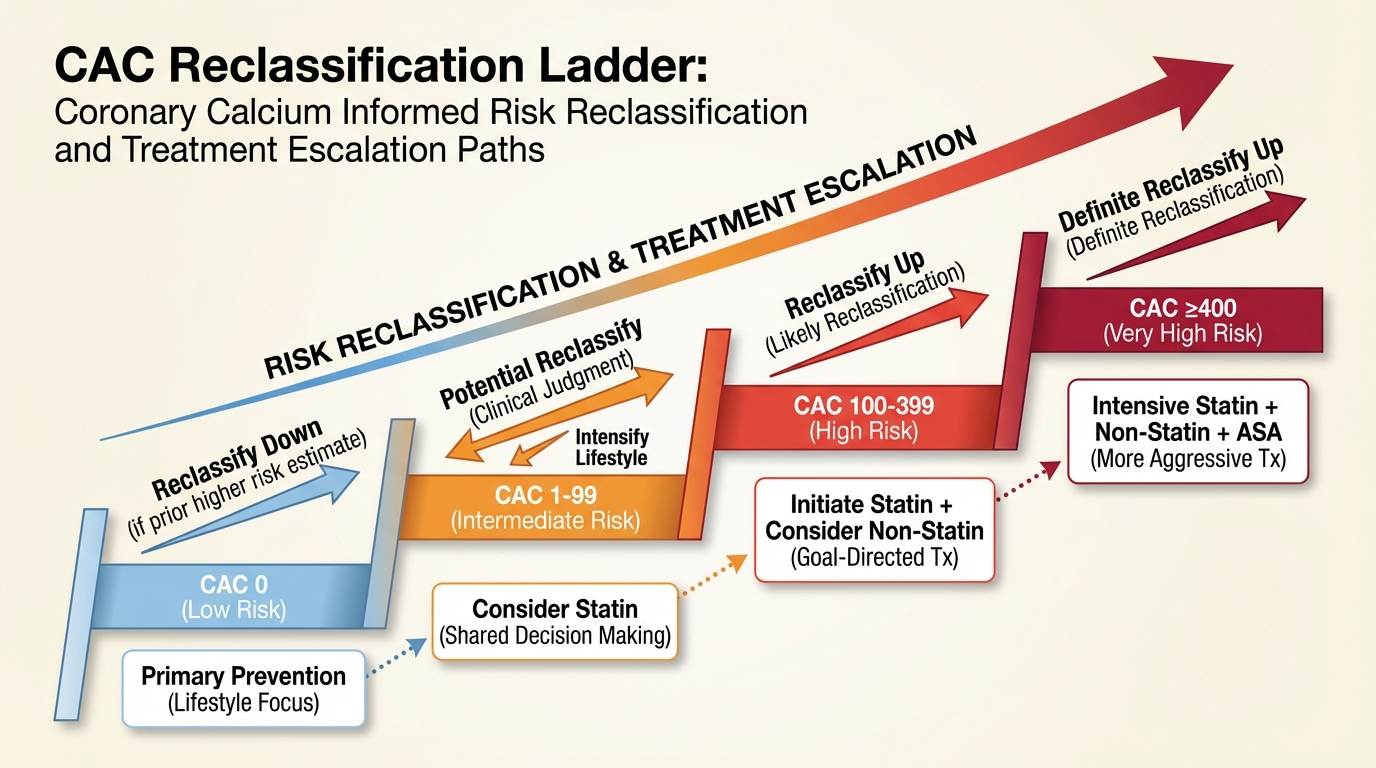
- More explicit reclassification logic using coronary calcium in uncertain cases.
LDL, ApoB, and Lp(a) in One Decision Frame
LDL remains a core treatment target, but apoB can better capture particle burden when triglycerides are elevated or discordance appears. Lp(a) identifies inherited risk that can justify earlier or more intensive prevention in otherwise borderline scenarios. The integration question is sequential: estimate baseline risk, identify hidden burden, then set treatment intensity that matches lifetime exposure profile.

CAC as Reclassification Tool
When uncertainty is high, coronary artery calcium can resolve treatment indecision by moving risk up or down in clinically meaningful ways. The main implementation risk is using CAC as a delay tactic rather than as a decision accelerator. If CAC is ordered, predefine how each result range changes the treatment plan.
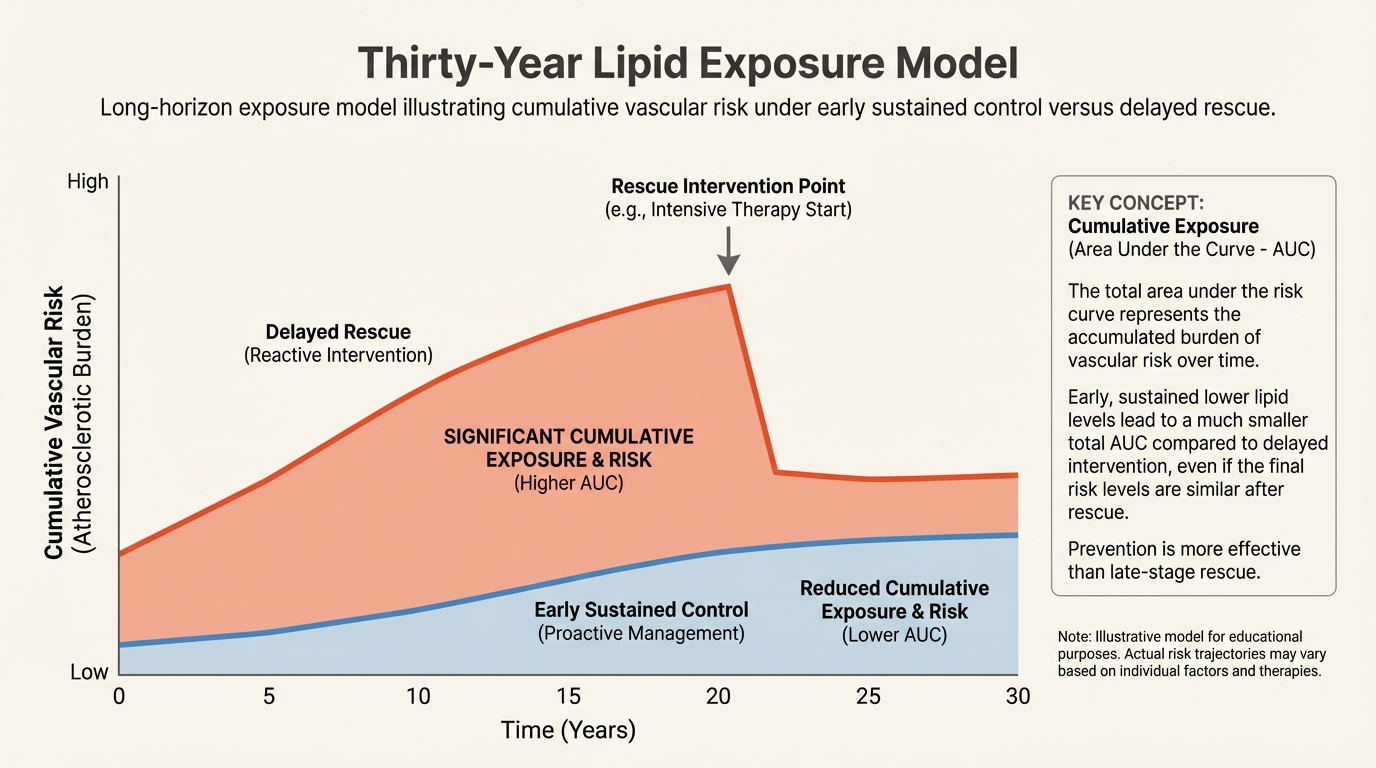
Why 30-Year Exposure Framing Matters
Short windows underprice cumulative vascular load in younger adults and in middle-aged adults with moderate but persistent elevation. Longevity medicine needs exposure accounting. Earlier sustained control can dominate late aggressive rescue in total-years-at-risk terms.
Operational Bottom Line
The 2026 update supports a more coherent prevention strategy: estimate risk with better equations, detect hidden burden with apoB and Lp(a), use CAC to resolve uncertainty, and optimize cumulative exposure rather than episodic numbers. This is a stronger framework for lifespan planning.
Source List
ACC/AHA guideline release summary (March 2026): AHA newsroom.
Professional guideline resource: Professional Heart Daily.
Lp(a) and lipid risk overview: American College of Cardiology resources.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.