Alzheimer Biomarkers Are Moving Faster Than Alzheimer Drugs
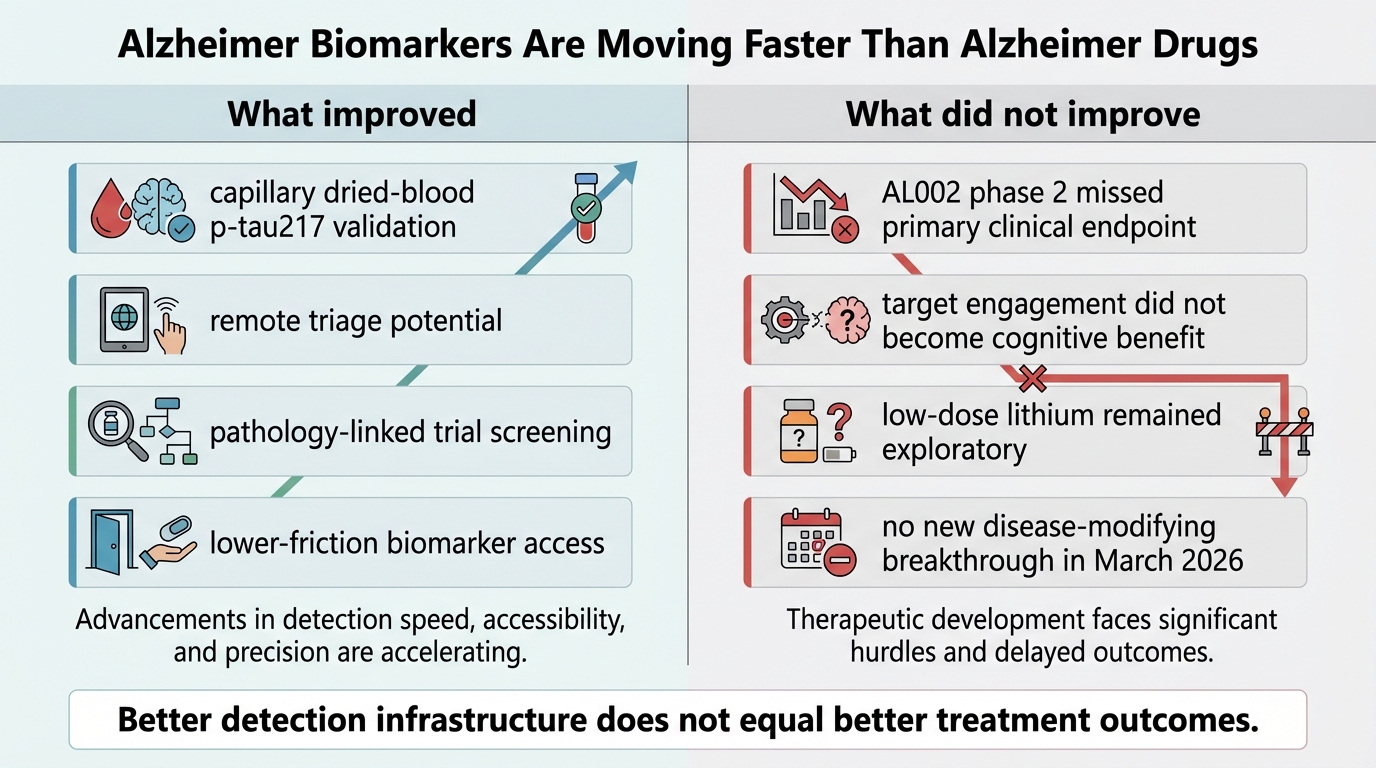
The March 2026 Alzheimer stack produced two different signals at once. Diagnosis and trial triage are becoming easier to scale. Therapeutic progress remains slower, less reliable, and harder to celebrate.
That split matters because it changes what a reasonable person should infer from the news flow. Blood biomarkers are genuinely improving the operational side of Alzheimer care. They are reducing friction around who should be evaluated, who should be referred, and who can be screened into research. That is established. It is not the same as saying the disease-modifying treatment problem is close to solved.
Core thesis: biomarker progress is real infrastructure progress. It improves detection, stratification, and trial design. It does not erase the fact that recent therapeutic results are still mixed or negative.
What Actually Improved
The strongest near-term advance is in access logic, not miracle treatment logic. In February 2026, Nature Medicine highlighted a dried-blood-spot workflow showing that capillary p-tau217, NfL, and GFAP measurements correlated with venous measures, and that capillary p-tau217 classified amyloid burden with useful accuracy. The underlying research paper reported an area under the curve of 0.863 for capillary p-tau217 against cerebrospinal-fluid biomarker status in a relevant subsample. That is not perfect equivalence with conventional workups, but it is good enough to matter for remote triage and large-scale screening.
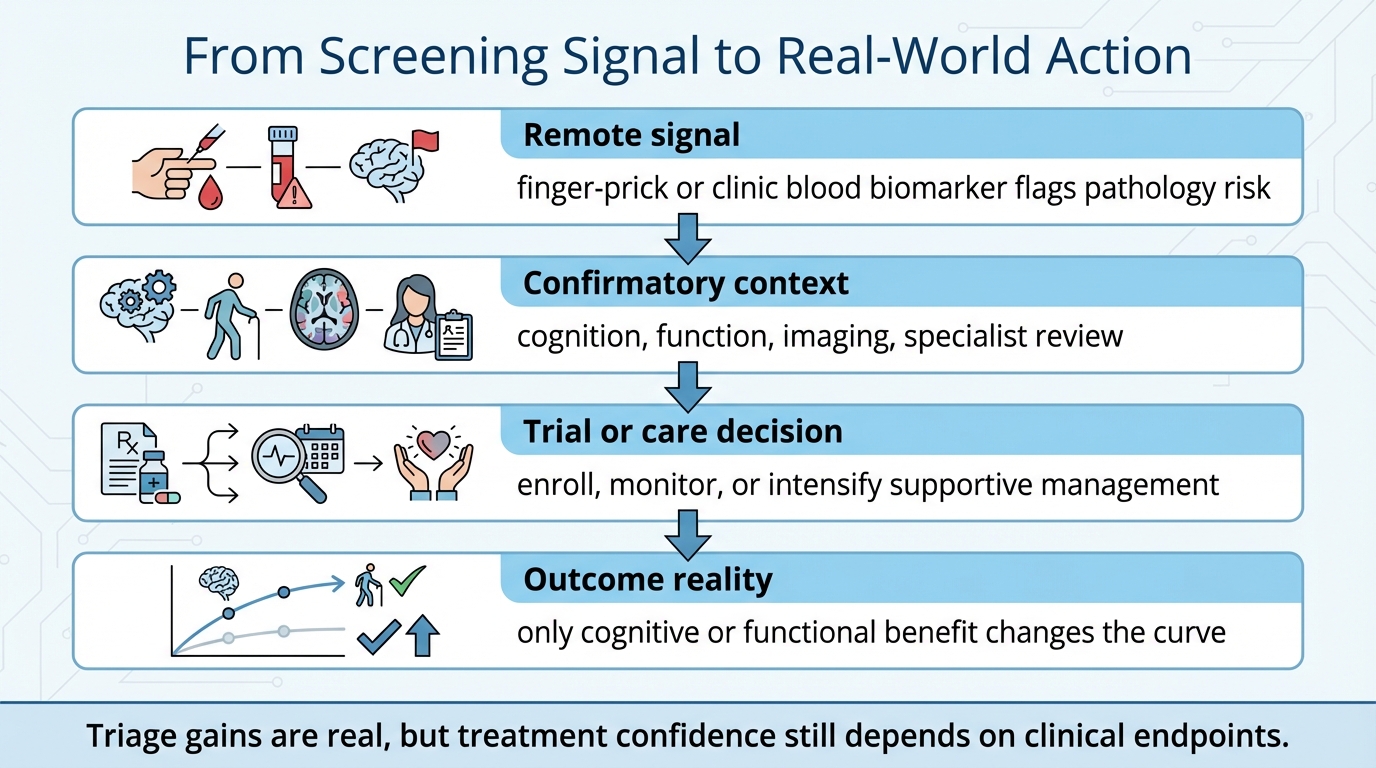
This is a practical shift. If pathology-linked blood tests become easier to collect outside specialist settings, the system can route the right people into confirmatory testing or trials faster. That lowers one of the old bottlenecks in Alzheimer care. It also strengthens the interpretation of earlier LifeMeter coverage on the primary-care blood-biomarker pivot, because March 2026 added more evidence that the collection layer itself can be simplified without abandoning pathology signal entirely.
Known fact: biomarker collection and classification are getting more scalable. Reasoned inference: this should improve trial enrollment efficiency and reduce some diagnostic delay. Unknown: how much of that operational improvement will translate into better real-world outcomes across fragmented care systems.
What Did Not Improve
The clearest new therapeutic read was discouraging. On March 5, 2026, Nature Medicine published the phase 2 randomized trial of the TREM2 agonistic antibody AL002 in early Alzheimer disease. The trial enrolled 381 participants, showed sustained target engagement in the central nervous system, and generated the sort of pharmacodynamic signal developers want to see. It still missed the primary endpoint of change in Clinical Dementia Rating-Sum of Boxes at week 96.
That result matters because it narrows the space for lazy optimism. This was not a case where nothing biological happened. Something did happen. Soluble TREM2 fell, osteopontin rose, and the drug clearly engaged the intended immune pathway. The disappointment is precisely that target engagement did not convert into a statistically significant clinical win. That is a more instructive failure than a completely inactive drug, because it shows again that mechanistic plausibility is not enough.
The treatment story also stayed modest in the better-looking smaller study. A March 2, 2026 pilot randomized clinical trial in JAMA Neurology tested low-dose lithium in older adults with mild cognitive impairment over two years. The trial established feasibility and tolerability, and one memory outcome moved in a favorable direction. But none of the six coprimary outcomes crossed the prespecified significance threshold. This is not a negative result in the same way as AL002, yet it is still not a basis for strong efficacy claims.
Why This Split Is Structurally Important
Biomarkers and treatments solve different problems. Biomarkers answer whether a patient likely has pathology, how advanced it may be, and whether a trial population is enriched enough to detect an effect. Treatments answer whether function or cognition is preserved. Confusing those roles produces bad headlines and worse decisions.
The Alzheimer field now has a stronger measurement layer than it had a few years ago. Blood tests, especially p-tau217-centered approaches, are pushing diagnosis and recruitment toward a lower-friction model. That is likely to make trial datasets cleaner. It may also reduce the number of patients who spend months in diagnostic limbo. None of that guarantees that a therapy hitting microglial or amyloid-linked biology will produce a clinically meaningful curve shift.
How To Read The March 2026 News Without Fooling Yourself
- Established: blood biomarker workflows are becoming easier to deploy, and capillary collection methods now have stronger validation than they had even a year ago.
- Established: AL002 produced target engagement without meeting its primary clinical endpoint in a reasonably sized phase 2 study.
- Established: low-dose lithium remains a feasibility and hypothesis-generating result, not a confirmed neuroprotective intervention.
- Inferred: better biomarker-driven recruitment should improve the efficiency of future therapeutic trials.
- Unknown: whether the next wave of mechanism-focused therapies will finally convert cleaner enrollment and earlier detection into durable cognitive benefit.
Why This Matters For Longevity Readers
Life extension discussions often treat neurodegeneration as if diagnosis and prevention can be merged into one continuous story. They cannot. A longevity-oriented reader should care about both early detection and intervention quality, but should not assign them the same evidentiary weight. A blood test that improves triage can change when you act. It does not prove that the action available is strong enough.
This distinction also affects personal planning. If family history, cognition concerns, or age trajectory make Alzheimer risk salient, the immediate benefit of better biomarkers is improved decision timing. You can clarify whether specialist evaluation, confirmatory testing, or trial enrollment deserves attention sooner. The longer-range challenge remains therapeutic scarcity. That is why prevention architecture, vascular risk control, sleep quality, exercise, and metabolic stability still matter so much. They are not substitutes for Alzheimer drugs. They are what remains actionable while the drug evidence continues to sort itself out.
For readers using LifeMeter as a decision layer, the practical move is not to chase every new therapeutic narrative. It is to use better testing only when it changes a concrete next step, and to keep the rest of the prevention stack grounded in stronger evidence categories. The biomarker pipeline is accelerating. The treatment pipeline has not yet earned the same confidence.
Decision Frame
| Question | Best current answer |
|---|---|
| Are Alzheimer blood biomarkers now more clinically usable? | Yes. The evidence for p-tau217-centered triage has strengthened, including in less invasive collection formats. |
| Did March 2026 deliver a new therapeutic breakthrough? | No. The highest-profile phase 2 result missed its primary endpoint, and the lithium pilot stayed exploratory. |
| Should biomarker progress change real behavior? | Yes, when it speeds specialist referral, confirmatory workup, or trial matching. No, if it is treated as proof that treatment risk has vanished. |
Further Reading Inside The Site
For the diagnostic side, see The Primary-Care Alzheimer’s Pivot and The Alzheimer’s Blood Test Era. For the broader prevention layer, the report funnel remains the same: use Biomarker Trend Analyzer for tracking discipline and the strategy report flow when you need a more integrated risk view.
Source List
Mummery CJ, et al. The TREM2 agonistic antibody AL002 in early Alzheimer’s disease: a phase 2 randomized trial. Nature Medicine. Published March 5, 2026.
Huber H, et al. A minimally invasive dried blood spot biomarker test for the detection of Alzheimer’s disease pathology. Nature Medicine. Referenced by research briefing published February 11, 2026.
Capillary blood sampling for detecting biomarkers of Alzheimer’s disease. Nature Medicine research briefing. Published February 11, 2026.
Gildengers AG, et al. Low-Dose Lithium for Mild Cognitive Impairment: A Pilot Randomized Clinical Trial. JAMA Neurology. Published online March 2, 2026.
Blood tests for Alzheimer’s disease could reshape research and care. Nature Medicine news analysis. Published February 5, 2026.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.