Plasma Dilution and Therapeutic Apheresis
The plasma-reset story became popular because it seemed to offer a shortcut around slow tissue repair. Change the circulating environment, remove the bad signals, and old biology may behave younger. That is not fantasy. It is also not the same as proving that human aging can be broadly reversed by apheresis. The mechanistic signal is real. The clinical proof remains narrow.
The first analytical mistake in this area is to collapse several different ideas into one claim. Heterochronic parabiosis, neutral blood exchange, therapeutic plasma exchange, and commercial apheresis protocols all sit on the same conceptual map, but they are not equivalent interventions. Some test whether old tissues respond to a changed systemic milieu. Some remove and replace plasma proteins. Some are established medical procedures used for autoimmune, neurologic, or hematologic indications. None of that, by itself, demonstrates a validated anti-aging therapy.
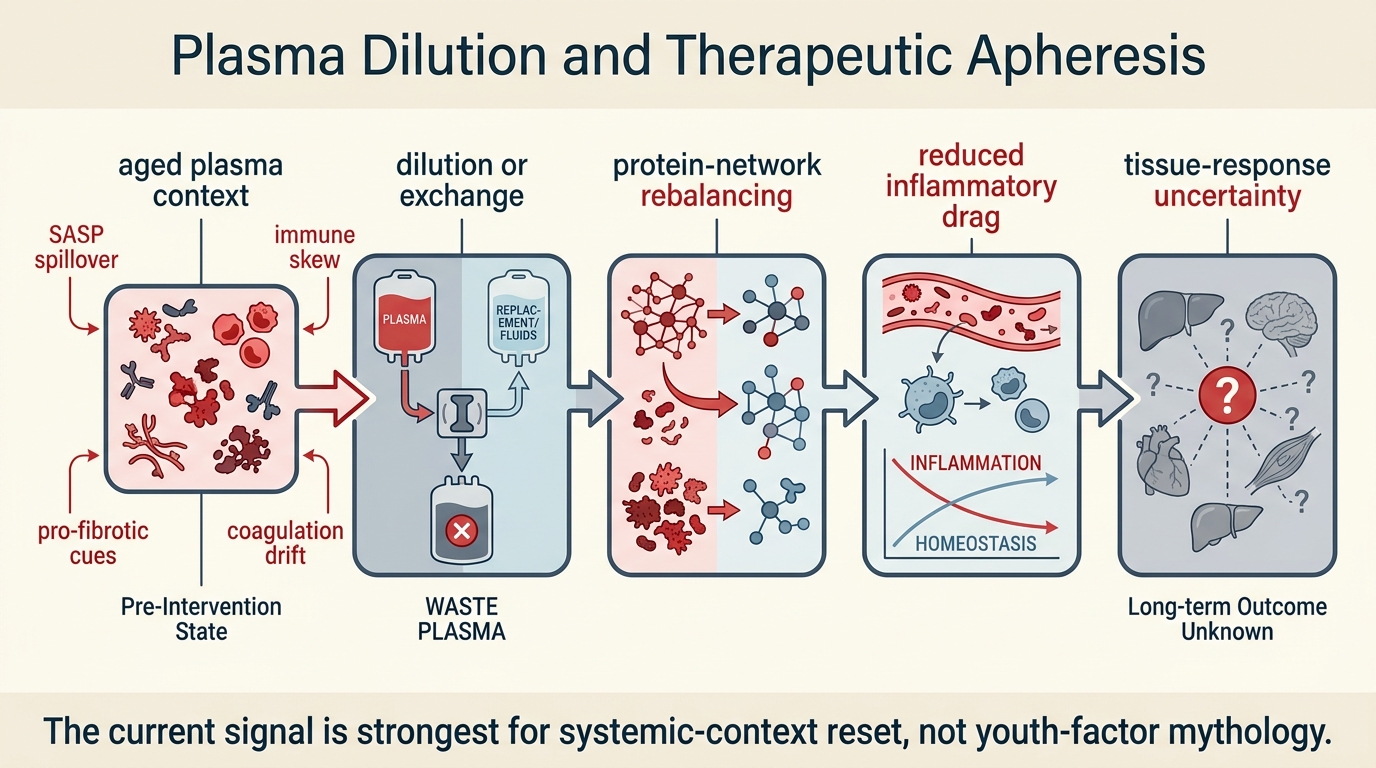
Core thesis: the strongest current signal is that the circulating environment matters more than many reductionist aging models once assumed. The most plausible mechanism is not transfer of youthful essence, but partial subtraction of pro-inflammatory, pro-fibrotic, or dysregulated plasma context. What remains unproven is whether that signal can be translated into durable, system-wide human rejuvenation rather than transient biomarker movement or disease-specific benefit.
What The Foundational Experiments Actually Show
Parabiosis experiments helped establish that aging is not only cell intrinsic. When old and young animals share circulation, some aging phenotypes shift. That observation created two competing stories. One story claimed youth factors in young blood drive repair. The other claimed old blood carries inhibitory factors, and reducing those burdens may matter at least as much. Later neutral-blood-exchange and plasma-dilution work made the second story harder to ignore.
That distinction matters because it changes the intervention logic. If youthful benefit depends on rare positive factors, then therapy should focus on replacement. If the dominant problem is a distorted protein and signaling environment, then subtraction, dilution, or selective removal becomes more plausible. The LifeMeter reading is that current evidence supports a mixed model, with more weight on rebalancing a damaged systemic environment than on importing a magical youth cargo.
Established fact ends there. The mouse signal does not tell us how broad the effect is in humans, how durable it would be, which tissues respond first, or whether benefit would come from one exchange, repeated exchange, albumin support, selective adsorption, or an entirely different plasma engineering approach. Those translation questions are still open.
Therapeutic Apheresis Is A Real Clinical Tool, But Not A General Longevity Therapy
Therapeutic plasma exchange already has legitimate medical uses. It can remove pathogenic antibodies, immune complexes, paraproteins, or other circulating components in defined disease settings. In those contexts the procedure is not speculative. It is part of standard care logic. That fact sometimes gets repurposed into a broader anti-aging narrative, but the leap is too large.
Using a validated procedure for one disease class does not establish its value for multi-system aging. Autoimmune crisis, hyperviscosity, and dysregulated aging are not interchangeable pathologies. The correct inference is narrower: apheresis proves that the bloodstream is a modifiable compartment and that changing circulating composition can alter physiology. It does not prove that broad, durable rejuvenation follows from that modulation.
Why The Mechanistic Story Still Deserves Serious Attention
The reason this area remains worth watching is that it fits a more system-level view of aging. Aging tissues accumulate not only DNA damage and cellular dysfunction, but also altered secreted signals, inflammatory mediators, clotting changes, fibrosis-promoting cues, and repair-suppressive states. A bloodstream that continuously carries those signals can act as an amplifier of decline. Interventions that reset that signaling environment could therefore have leverage across multiple tissues at once.
This is one reason the topic connects naturally to Stem Cell Exhaustion and Replenishment Strategies. Stem-cell decline is not just a problem inside the cell. It is also a problem of niche quality, inflammatory load, and repair instruction. Plasma interventions are interesting because they target part of that environment rather than only the cell population.
Where The Human Evidence Is Still Thin
The main limitation is not that nothing happens in humans. It is that the endpoints that matter most for aging remain underdeveloped. The field needs repeated-measure evidence on functional outcomes, not only transient biomarker shifts. That means muscle performance, aerobic capacity, frailty trajectories, inflammatory burden over time, immune function, and disease-relevant durability. A short-term protein-profile change is interesting. It is not enough.
There is also a design problem. Plasma interventions are difficult to standardize. Exchange volume, replacement fluid, albumin concentration, frequency, patient selection, baseline inflammatory state, and concurrent therapy can all change the effect. That makes small uncontrolled programs easy to oversell and hard to compare. It also means that one clinic's protocol tells you very little about another clinic's claims.
What Would Count As Real Translation
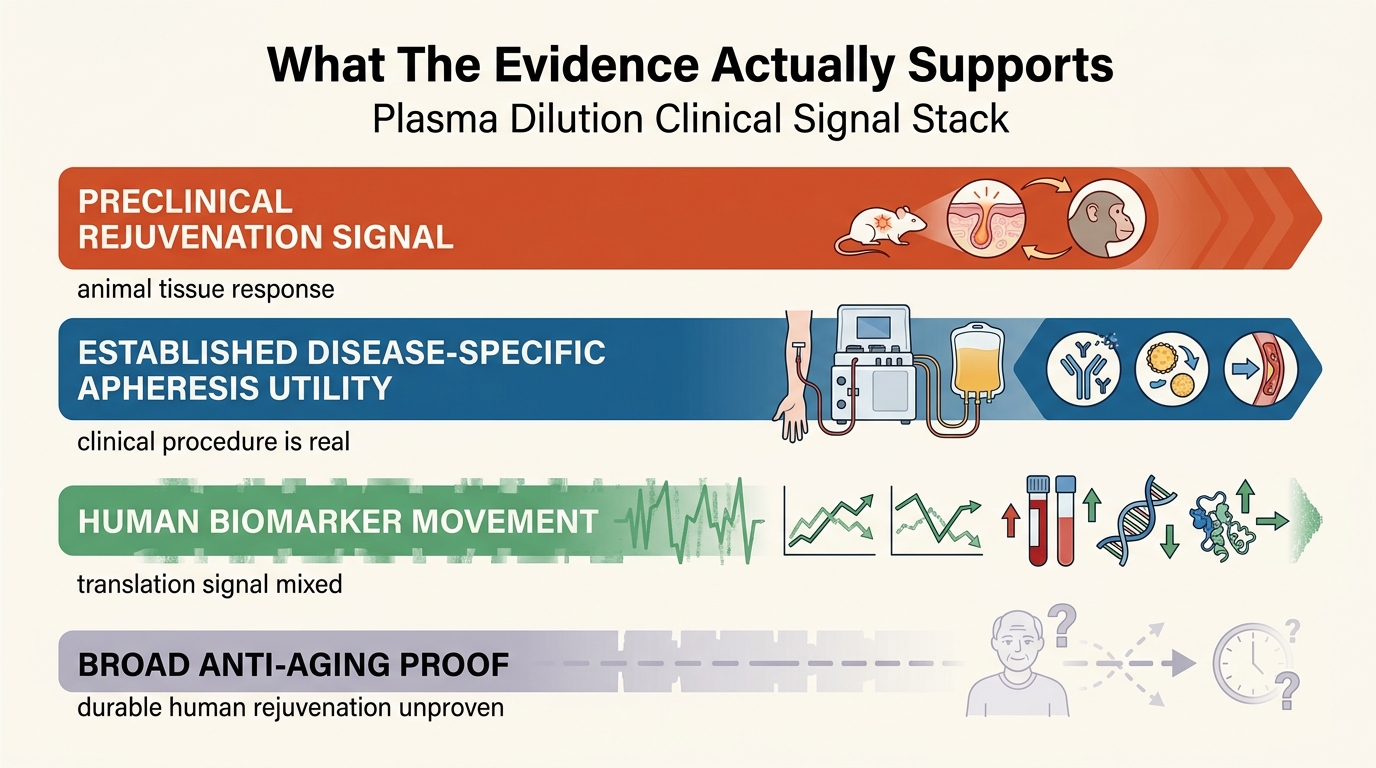
- Strong evidence: replicated improvement in functional aging endpoints with clear protocol description and tolerable repeat-use safety.
- Intermediate evidence: reproducible biomarker and inflammatory-signal shifts that correlate with better tissue function.
- Weak evidence: one-off clinic experiences, marketing language around detox or youth plasma, and vague vitality claims without comparator design.
This is why the correct stance is neither dismissal nor hype. Plasma dilution should not be treated as established rejuvenation medicine. It also should not be dismissed as biologically unserious. It belongs in the same bucket as several other high-interest longevity interventions: credible systems logic, meaningful preclinical signal, incomplete translation, and a large gap between what laboratories suggest and what clinics can responsibly claim.
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | Animal work supports the idea that changing the circulating environment can alter aging-related tissue behavior. |
| Known | Therapeutic plasma exchange is an established clinical procedure for several non-aging indications and proves that plasma composition is modifiable. |
| Known | Current human evidence does not establish broad rejuvenation, lifespan extension, or durable multi-system anti-aging benefit from apheresis. |
| Inferred | The most plausible leverage point is partial removal or rebalancing of harmful circulating context rather than simple transfer of youth-promoting factors alone. |
| Unknown | Which human subgroups, dosing schedules, replacement strategies, and outcome measures would translate the mechanistic signal into durable clinical value. |
The Practical Reading For Longevity Operators
If you are evaluating this field as an informed outsider, the correct question is not whether plasma exchange is real. It is whether a specific protocol can show reproducible benefit on meaningful aging endpoints without relying on narrative inflation. That means asking for patient selection criteria, exchange details, replacement composition, follow-up duration, comparator logic, and functional outcomes. Most public claims do not meet that standard yet.
The deeper lesson is that aging is partly systemic and circulatory, not only cellular. The field may advance through selective plasma engineering, targeted adsorption, better inflammatory-protein mapping, or combination approaches that pair systemic reset with tissue-specific repair. Plasma dilution may be less the final therapy than the clue that the blood compartment has been under-modeled.
Further Reading Inside The Site
This article connects directly to Stem Cell Exhaustion and Replenishment Strategies, Senolytics Moving into Clinical Translation, and Longevity Clinics: Science, Protocols, and Variability. Together they frame the difference between plausible repair logic and decision-grade human evidence.
Source List
Conboy IM, Conboy MJ, Wagers AJ, et al. Rejuvenation of aged progenitor cells by exposure to a young systemic environment. Nature. 2005.
Mehdipour M, Skinner C, Wong N, et al. Rejuvenation of three germ layers tissues by exchanging old blood plasma with saline-albumin. Aging. 2020.
Padmanabhan A, Connelly-Smith L, Aqui N, et al. Guidelines on the use of therapeutic apheresis in clinical practice. Journal of Clinical Apheresis. American Society for Apheresis.
Villeda SA, Plambeck KE, Middeldorp J, et al. Young blood reverses age-related impairments in cognitive function and synaptic plasticity in mice. Nature Medicine. 2014.
Model the capital side of a long-horizon intervention strategy.
Open the paired WealthMeter scenario with a reserve-sensitive balance sheet so the biology question and the funding question can be evaluated together.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.