Off-Label Longevity Prescriptions: Risks and Patterns
A patient does not care whether a prescription sits inside a neat regulatory category. The patient cares whether the drug is likely to help, what is actually known, who is watching for harm, and whether the story being sold is stronger than the evidence underneath it. Longevity medicine has a habit of collapsing those questions into one soft phrase: off-label. That shortcut hides more than it explains.
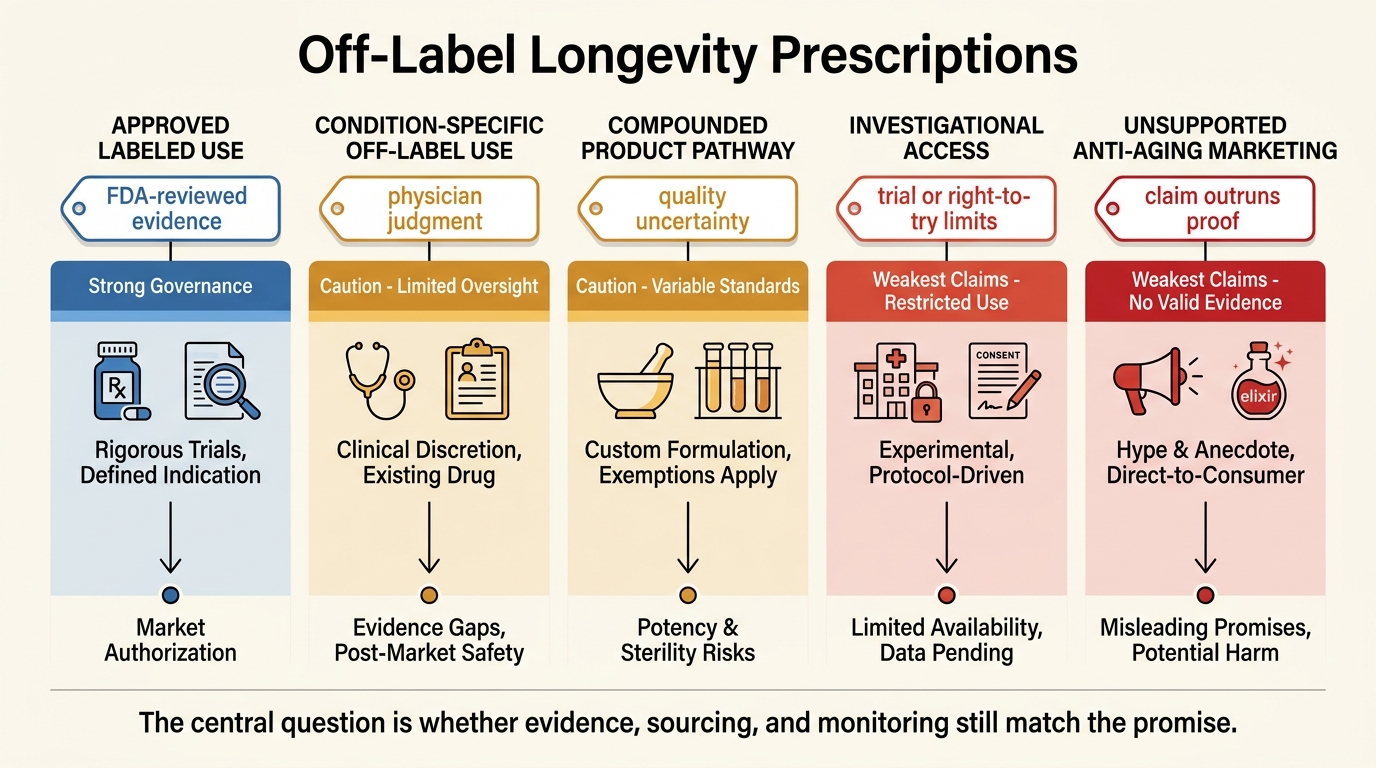
Established fact: once an FDA-approved drug is on the market, clinicians may generally prescribe it for an unapproved use when they judge that use medically appropriate for a patient. Established fact: FDA approval does not extend automatically to that new use, which means the evidence, dosing logic, monitoring plan, and risk-benefit balance may be much less certain. In longevity practice, the gap matters because the field often mixes legitimate physician discretion with weaker anti-aging narratives, compounded products, and a marketing style that makes uncertainty look like frontier sophistication.
Core thesis: off-label prescribing is not itself a red flag. The red flags appear when a clinic treats off-label status as evidence of being ahead of the science, blurs the line between approved drugs and unapproved compounded products, or sells a generalized anti-aging promise without a condition-specific evidence stack and monitoring plan.
Off-Label Does Not Mean Illegal Or Reckless
The first correction is simple. Off-label use of an approved drug is ordinary medicine. Oncology, pediatrics, rare disease care, and many other fields use off-label prescribing when the approved label is narrower than actual clinical need. FDA itself explains this directly. The approved label tells clinicians that the agency reviewed the benefit-risk evidence for a particular use. It does not prevent clinicians from using the drug in other ways when they judge the situation warrants it.
The second correction is more important for longevity readers. Lawful prescribing discretion does not turn a weak evidence base into a strong one. It only means the regulatory system allows a clinician to make a judgment call. The quality question remains separate: what human data support the use, how transferable is the mechanistic logic, what monitoring is needed, and what harms become more plausible when treatment shifts from disease management into multi-year preventive or enhancement framing?
Why Longevity Clinics Reach For Off-Label Protocols
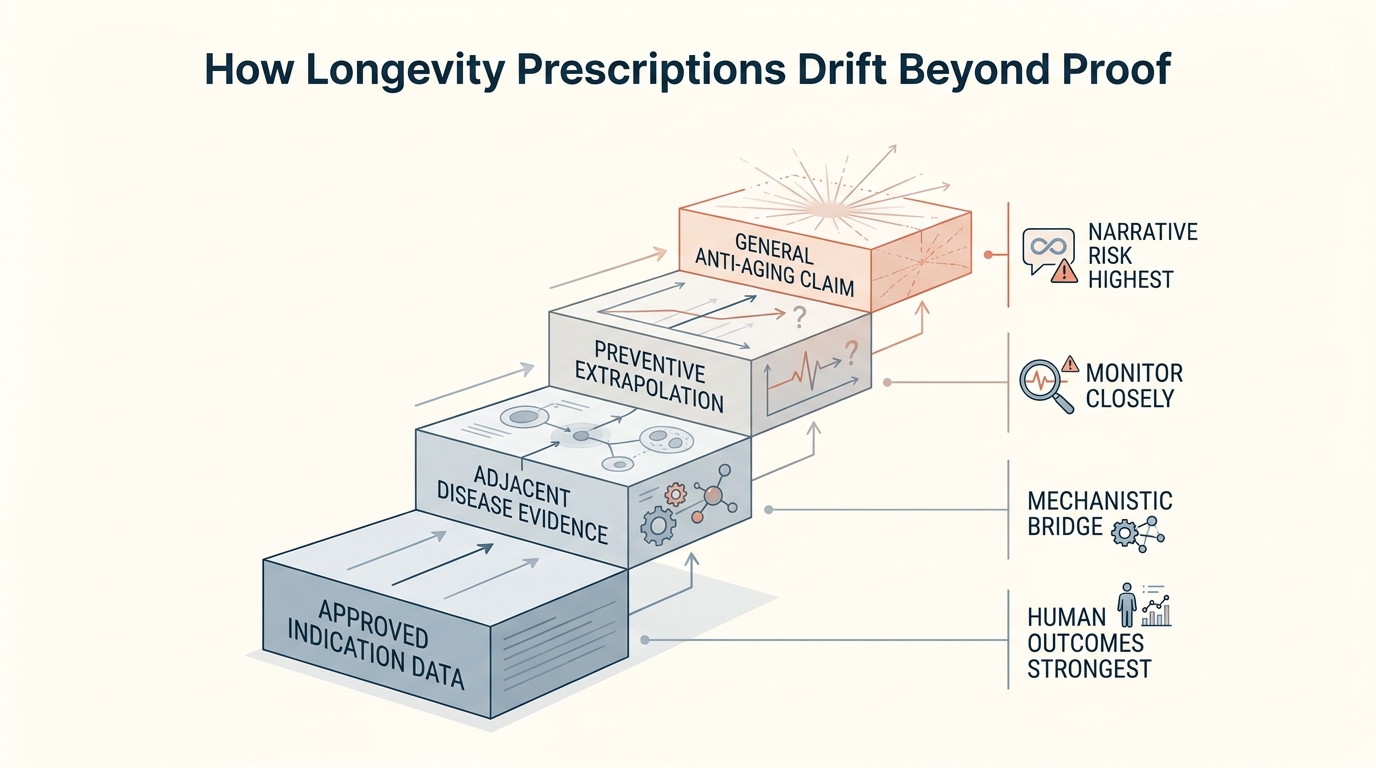
The structural reason is not mysterious. Aging itself is not treated as a standard FDA indication, so many interventions that attract interest in longevity are discussed through adjacent disease labels, biomarker endpoints, body-composition changes, or symptom clusters rather than through an approved anti-aging claim. That leaves a wide space in which clinicians and clinics can say, in effect, that they are using familiar drugs for a different strategic goal.
Some of those uses may be reasonable in narrow cases. A patient with metabolic disease, inflammatory burden, or severe risk-factor clustering can overlap partially with a longevity-oriented goal. The problem starts when that narrow overlap becomes a general protocol template. Mechanistic plausibility is then treated as if it were durable human outcome evidence, and heterogeneous patients are grouped under one aspirational banner.
The Three Patterns That Usually Deserve The Most Skepticism
The first is evidence stretching. A clinic cites disease-specific or short-duration data, then quietly extends the story into general rejuvenation, slower biological aging, or prevention of future decline. That is an inference, not a demonstrated result. Sometimes it is a reasonable research hypothesis. It is not the same thing as a decision-grade proof base for routine prescribing.
The second is pathway confusion. Approved off-label use of a manufactured FDA-approved drug is not the same as a compounded preparation. FDA states clearly that compounded drugs are not FDA-approved and that the agency does not review them for safety, effectiveness, or quality before they reach patients. Longevity discussions often glide over that distinction. A patient hears about one molecule and assumes all versions carry the same governance. They do not.
The third is category blending. Clinics may mention off-label prescribing, compounding, investigational access, and right-to-try in the same breath, as if they are interchangeable forms of innovation. They are not. Right to Try applies only to certain investigational products for patients with life-threatening disease who meet statutory criteria. Expanded access and clinical trials have their own structures. Off-label use applies to already approved drugs. Treating these categories as one frontier stack is usually a sign that the sales narrative is outrunning the governance reality.
The Real Risk Is Often Governance Failure, Not One Molecule
Many longevity prescriptions do not fail because the molecule is obviously absurd. They fail because the surrounding decision system is weak. Baseline diagnosis may be loose. Outcome targets may be vague. Adverse-effect monitoring may be irregular. Interactions across multi-drug protocols may be under-modeled. Stopping rules may be unclear. A clinic can therefore offer a sophisticated-looking regimen while still operating without the discipline that would make long-horizon use defensible.
This is one reason longevity medicine produces so much disagreement between mechanistic enthusiasts and more conservative clinicians. The enthusiast often focuses on pathway plausibility. The conservative reader asks a different question: what happens when a drug meant for one risk frame is moved into broad preventive use in relatively healthy people, over longer durations, with variable product sourcing and incomplete comparative evidence? That second question is where many anti-aging protocols start to look much weaker.
What A Stronger Off-Label Case Looks Like
- A defined clinical problem. The prescription is tied to a specific condition, measurable risk state, or credible therapeutic objective rather than a vague ambition to age better.
- An evidence ladder. The clinician can explain what is known from approved use, what is borrowed from adjacent populations, and what remains inferential.
- A product-pathway check. The patient knows whether the drug is the FDA-approved product, a compounded variant, or an investigational product under a separate pathway.
- A monitoring and stopping plan. Labs, symptom checks, adverse-effect surveillance, and discontinuation thresholds are specified in advance.
- Constraint in the claim. The clinician does not imply that an off-label use is an evidence-backed longevity therapy when the actual support is narrower.
That last point matters because the market reward for sounding ahead of the evidence is high. A disciplined clinician should sound less impressive than the clinic that promises broad anti-aging optimization through a stack of frontier protocols. In this domain, restraint is often a positive signal.
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | FDA-approved drugs may generally be prescribed off-label by clinicians, but FDA has not determined those unapproved uses to be safe and effective for the new indication. |
| Known | Compounded drugs are not FDA-approved, and the agency warns that they are not reviewed for safety, effectiveness, or quality before marketing. |
| Known | Right to Try is a narrow statutory pathway for eligible investigational drugs in patients with life-threatening disease, not a general longevity-access route. |
| Inferred | The most common weakness in longevity off-label prescribing is not always the molecular rationale itself, but the extension from narrow or adjacent evidence into generalized preventive promise without equally strong monitoring and governance. |
| Unknown | Which current off-label longevity protocols will show durable net human benefit once multi-year follow-up, broader populations, product-pathway differences, and comparative safety are measured directly. |
The Practical Reading For Patients And Clinicians
The right question is not, “Is this off-label?” The right sequence is: what is the actual problem being treated, what evidence directly supports that use, what parts are mechanistic inference, what product pathway is being used, and what monitoring discipline makes the risk tradeoff acceptable? If a clinic cannot answer those questions cleanly, the prescription may be less a therapeutic decision than a frontier-branded wager.
Longevity medicine will keep using off-label tools because the regulatory map for aging is still narrow. That does not make the field unserious. It does mean the burden of honesty is higher. When the label does not carry the claim, the clinician has to carry more of the proof burden, more of the surveillance burden, and more of the explanatory burden. That is the standard serious readers should apply.
Further Reading Inside The Site
This article connects directly to Regulatory Barriers to Anti-Aging Drugs, Longevity Clinics: Science, Protocols, and Variability, and Plasma Dilution and Therapeutic Apheresis. Together they show why translational ambition only becomes credible when the evidence, product pathway, and patient-governance logic remain aligned.
Source List
U.S. Food and Drug Administration. Understanding Unapproved Use of Approved Drugs “Off Label”. Accessed May 4, 2026.
U.S. Food and Drug Administration. Right to Try. Accessed May 4, 2026.
U.S. Food and Drug Administration. Human Drug Compounding. Accessed May 4, 2026.
U.S. Food and Drug Administration. Human Drug Compounding Laws. Accessed May 4, 2026.
U.S. Food and Drug Administration. FD&C Act Provisions that Apply to Human Drug Compounding. Accessed May 4, 2026.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.