Closed-Loop Longevity Systems: Measure, Intervene, Adapt
The closed-loop dream in longevity is simple to describe and hard to execute. Measure the body, change the inputs, observe the response, then adapt the plan before damage compounds. The difficulty is that aging is not a single-variable control problem, most useful endpoints move slowly, and many measurements are still proxies rather than decision-grade readouts.
Established fact comes first. Closed-loop medicine already exists in narrow settings where the signal is fast, the intervention is specific, and the consequence of error is measurable. Automated insulin delivery is the clearest example. Certain intensive-care and ventilatory systems also use repeated measurement and adjustment. The control loop works there because the causal chain is comparatively tight.
Longevity is broader. It pulls together metabolic regulation, inflammation, sleep, fitness, body composition, vascular risk, drug response, and tissue-specific decline. That makes the phrase closed-loop longevity more of a research program than a finished product. What exists today is a spectrum that runs from disciplined feedback systems to glossy dashboards with weak causal power.
What the Loop Actually Requires
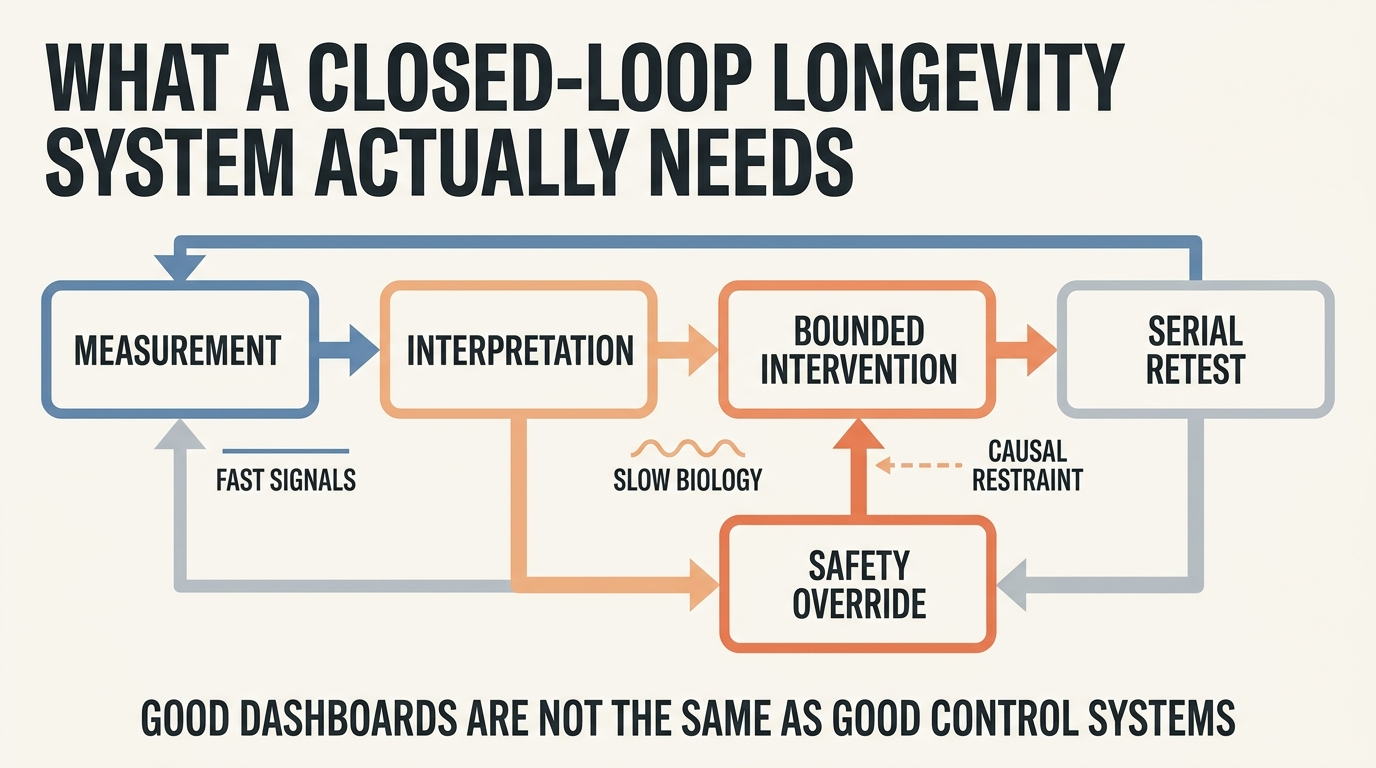
A real control loop needs five parts. First, a measurement that is repeatable enough to distinguish signal from noise. Second, an interpretation layer that does not confuse correlation with mechanism. Third, an intervention that can be changed in a bounded way. Fourth, a retest interval that matches the biology. Fifth, a safety rule that stops the system from escalating on the basis of weak evidence.
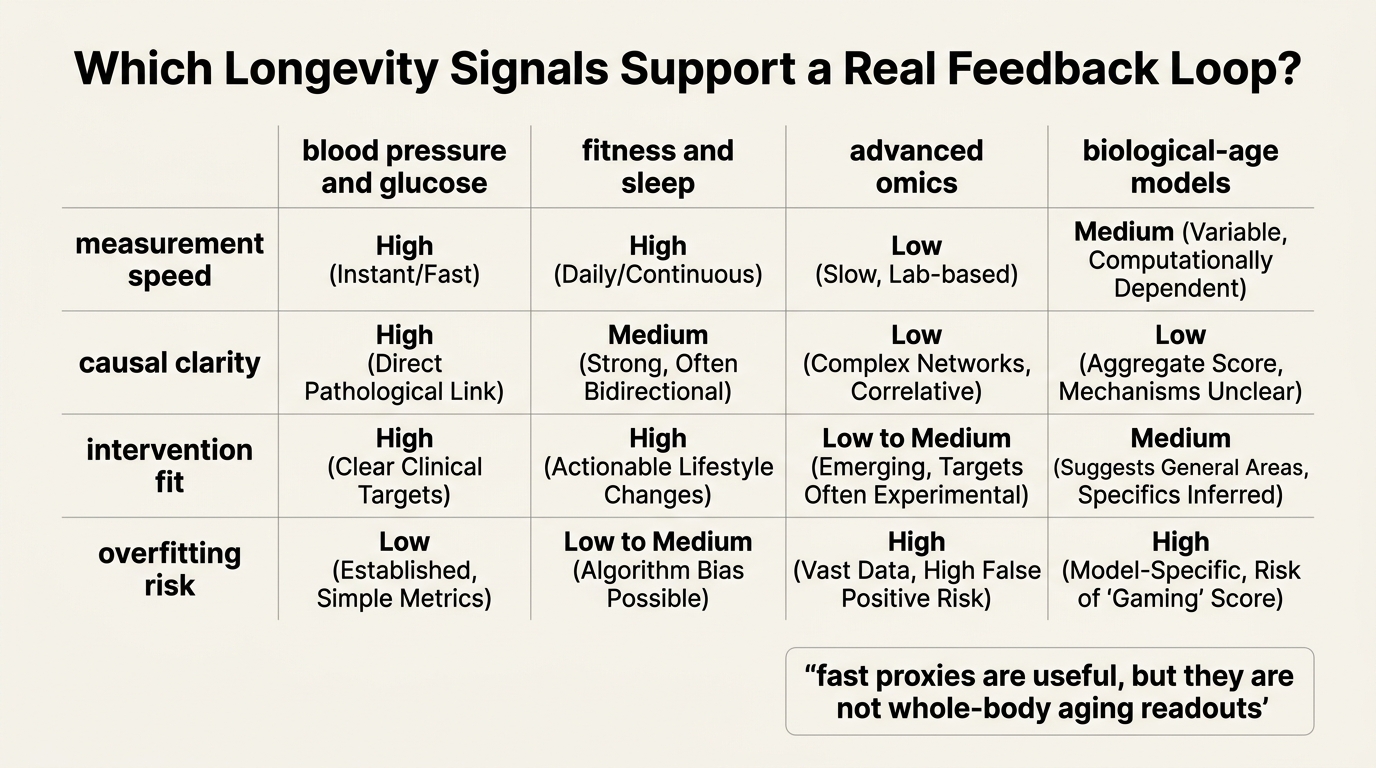
The measurement problem is where most longevity systems fail first. Wearables can capture heart rate, sleep, activity, temperature trend, and sometimes glucose or rhythm features. Labs can capture apoB, HbA1c, fasting insulin, inflammatory markers, kidney function, liver function, and other risk signals. Research tools can go further into epigenetic clocks, proteomics, metabolomics, and composite biological-age models. None of that means a consumer system can infer whether one supplement, one fasting schedule, or one repurposed drug altered the pace of aging itself.
Established: serial biomarkers can improve risk tracking and intervention monitoring.
Inference: the same data stream can support a full anti-aging control system only when the intervention-response link is much tighter than it usually is today.
Where the Measurement Layer Is Strongest
The strongest current loop is cardiometabolic. Blood pressure, continuous or repeated glucose data, body composition, resting fitness markers, sleep duration, medication adherence, and standard lab panels can all move on a timescale that is clinically usable. That does not solve aging, but it does control several high-value risk contributors to late-life decline.
This is where articles such as Insulin Sensitivity as a Longevity Lever, Biomarkers for Senescent Cell Burden, and Multi-Omics Integration: From Data to Intervention connect. Insulin sensitivity can be tracked well enough to guide diet, exercise, sleep, and sometimes medication. Senescent burden cannot. Multi-omics can sharpen discovery and stratification, but it still needs a clinical bridge before it becomes a trustworthy day-to-day control variable.
The weak zones are just as important. Epigenetic age estimates can be informative in serial use, but they are still model outputs rather than direct mechanistic readouts. Proteomic and metabolomic panels can reveal useful shifts, but they also raise multiple-comparison and interpretation problems. A loop is only as good as its least reliable decision variable.
Why Most Interventions Break the Loop
The intervention side is not clean either. Exercise volume changes several systems at once. Sleep improvement changes appetite, insulin action, training recovery, and blood pressure. Weight loss changes inflammation, glucose control, joint load, and hormone signaling. Those are desirable effects, but they make attribution difficult. The loop often sees a portfolio shift, not one isolated input.
Drug-based longevity claims create a different problem. Repurposed agents such as metformin, rapamycin analogs, senolytics, or NAD-focused compounds come with heterogeneous evidence bases, dose uncertainty, interaction risk, and endpoint ambiguity. A system that reacts aggressively to a small biomarker move can create false precision around interventions whose long-horizon benefit remains unsettled.
| Loop Component | What Is Strong Today | What Still Fails |
|---|---|---|
| Measurement | Blood pressure, glucose patterns, lipids, body composition, sleep, fitness trend | Whole-body aging burden, tissue repair quality, true biological-age causality |
| Interpretation | Risk-factor management and adherence feedback | Attribution of one intervention to broad longevity claims |
| Intervention | Diet, exercise, sleep, medication titration, weight management | Confident optimization of experimental anti-aging stacks |
| Adaptation cadence | Weeks to months for metabolic and cardiovascular markers | Fast iteration on slow aging endpoints without overfitting noise |
What a Serious System Would Look Like
A credible longevity loop would be conservative by design. It would separate fast operational markers from slow structural markers. It would use strong priors instead of treating every new data point as equally meaningful. It would demand repeated confirmation before changing a plan. It would also force the user to state what the intervention is trying to improve: glycemic stability, cardiorespiratory fitness, sleep architecture, body composition, medication tolerance, or a specific risk marker.
That is why the future likely belongs to layered systems rather than a single master dashboard. A useful stack may combine wearable recovery trend, conventional laboratory monitoring, selective imaging or specialist assessment, and a limited set of advanced biomarkers used for context rather than for theatrical certainty. The loop becomes practical when each layer has a defined role.
This is also where network biology and AI-guided drug discovery may matter most. Their short-run value is likely to improve model selection, risk stratification, and intervention ranking before they deliver any clean autonomous anti-aging control system.
What Is Known, Inferred, and Still Unknown
Known: repeated measurement improves many forms of preventive medicine, especially when the target is cardiometabolic risk, treatment adherence, or training and recovery management. Known: aging biology is distributed across multiple systems and timescales. Known: biomarkers differ sharply in specificity, stability, and translational usefulness.
Inferred: the first generation of real longevity loops will come from disciplined management of high-leverage risk systems rather than from a universal anti-aging operating system. Inferred: hybrid stacks that combine conventional medicine with selected advanced biomarkers will outperform dashboard-heavy, mechanism-light consumer products.
Unknown: whether any broad biological-age loop can become responsive, causal, and safe enough for high-frequency adaptation. Unknown: which advanced markers will prove robust under real-world serial use. Unknown: how many intervention classes will remain too slow or too confounded for genuine loop control.
Sources and Evidence Frame
Established claims in this article rely on the mature literature around closed-loop control in diabetes and intensive monitoring settings, along with the larger evidence base on cardiovascular and metabolic risk-factor management, wearable measurement limits, and biomarker heterogeneity in aging research.
Interpretive claims are narrower. The argument is that longevity control will emerge first through layered risk management and only later, if at all, through a general anti-aging optimization loop. That is a reasoned inference from the current state of measurement and intervention quality rather than a settled fact.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.