Combination Therapies: Why Single-Drug Approaches Fail
People do not age in neat, isolated failure modes. A patient can lose muscle, accumulate senescent burden, drift into insulin resistance, and pick up vascular or neuroinflammatory damage at the same time. That is why the dream of one clean anti-aging drug keeps colliding with biology that is not built around one bottleneck.
The case for combination therapy is therefore not marketing exuberance. It follows from the structure of the problem. Aging expresses through interacting layers of damage, compensation, and tissue-specific decline. A drug that improves one pathway may still leave enough of the rest untouched that the whole-person outcome barely moves. The real question is not whether combination logic is philosophically attractive. It is where that logic is already justified, and why proving it in humans remains so hard.
Established fact: aging involves multiple partially interacting processes rather than one universally accepted master lesion. Reasoned inference: because several layers can remain limiting at once, durable clinical benefit will often require multi-agent or multi-modal intervention rather than a single-pathway win.
Why Single-Agent Logic Breaks Down
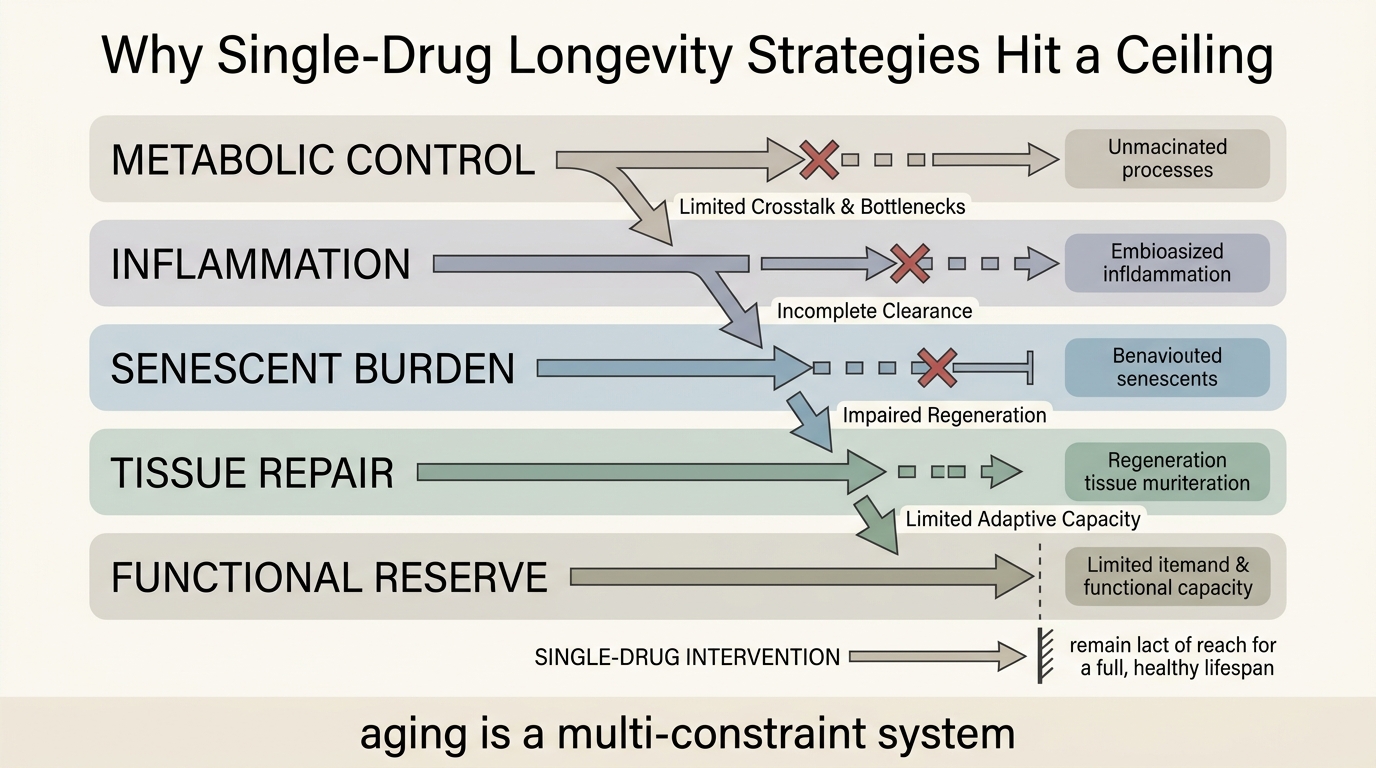
Single-drug thinking works best when disease has one dominant driver, one decisive pathway, or one short causal chain between mechanism and outcome. That pattern appears in infectious disease more often than in aging. Longevity medicine faces a broader systems problem: nutrient sensing, mitochondrial quality, immune surveillance, extracellular matrix integrity, stem-cell reserve, and chronic inflammatory signaling can all matter at once, but not equally in every tissue.
This does not mean every aging article must invoke total complexity. It means the ceiling on single-agent impact is usually lower than people want to admit. A senolytic may reduce one burden. A GLP-1 therapy may improve cardiometabolic risk. An exercise protocol may protect muscle and glycemic control. None automatically rewrites cognitive aging, fibrosis, immune exhaustion, or organ-specific repair capacity. The most persuasive longevity framework is therefore layered rather than singular.
Where Combination Logic Is Strongest
Combination thinking is strongest when the intervention targets clearly distinct but complementary constraints. One layer might reduce incoming damage. Another might improve clearance of existing burden. A third might preserve function while repair catches up. In oncology, infectious disease, hypertension, and HIV treatment, medicine already accepts this pattern because the target is too adaptive or too multi-causal for one lever to dominate. Aging has different biology, but the structural lesson carries over.
The logic is especially strong when no single intervention fixes the exposure-response chain from molecular damage to whole-organ function. That is why readers should connect this topic to LifeMeter pieces on network biology, tissue-specific senescence, and compression of morbidity. All three point to the same conclusion: localized wins can be real without being system-wide wins.
| Intervention layer | Main job | Why another layer may still be needed |
|---|---|---|
| Metabolic control | Reduce glycemic stress, adiposity burden, and some inflammatory signaling | Does not directly clear senescent cells, rebuild matrix, or restore lost tissue architecture |
| Damage clearance | Lower burden from dysfunctional or pro-inflammatory cells | Does not automatically restore stem-cell reserve or rebuild organ-specific structure |
| Repair or regeneration | Improve local tissue function or replacement capacity | May fail if upstream inflammatory or metabolic stress remains high |
| Behavioral platform | Exercise, sleep, protein adequacy, and adherence stability | Provides system support but may not reverse deeper pathological burden alone |
Why Human Translation Gets Hard Fast
The case for combination therapy is easier to state than to validate. Trial design becomes expensive because each added agent expands dosing questions, sequencing questions, interaction risk, and endpoint ambiguity. If a combination improves one biomarker while worsening tolerability, did the regimen work? If two modest agents together improve function, which piece mattered? If a program shows benefit only in a narrow phenotype, was the logic wrong or only the inclusion criteria?
Those problems are not excuses to retreat into single-drug simplicity. They are the real operational constraints. Combination longevity medicine will probably advance first in settings where individual components already have independent safety records, where endpoint logic is clinically legible, and where the combination is anchored to a specific population rather than sold as universal anti-aging medicine.
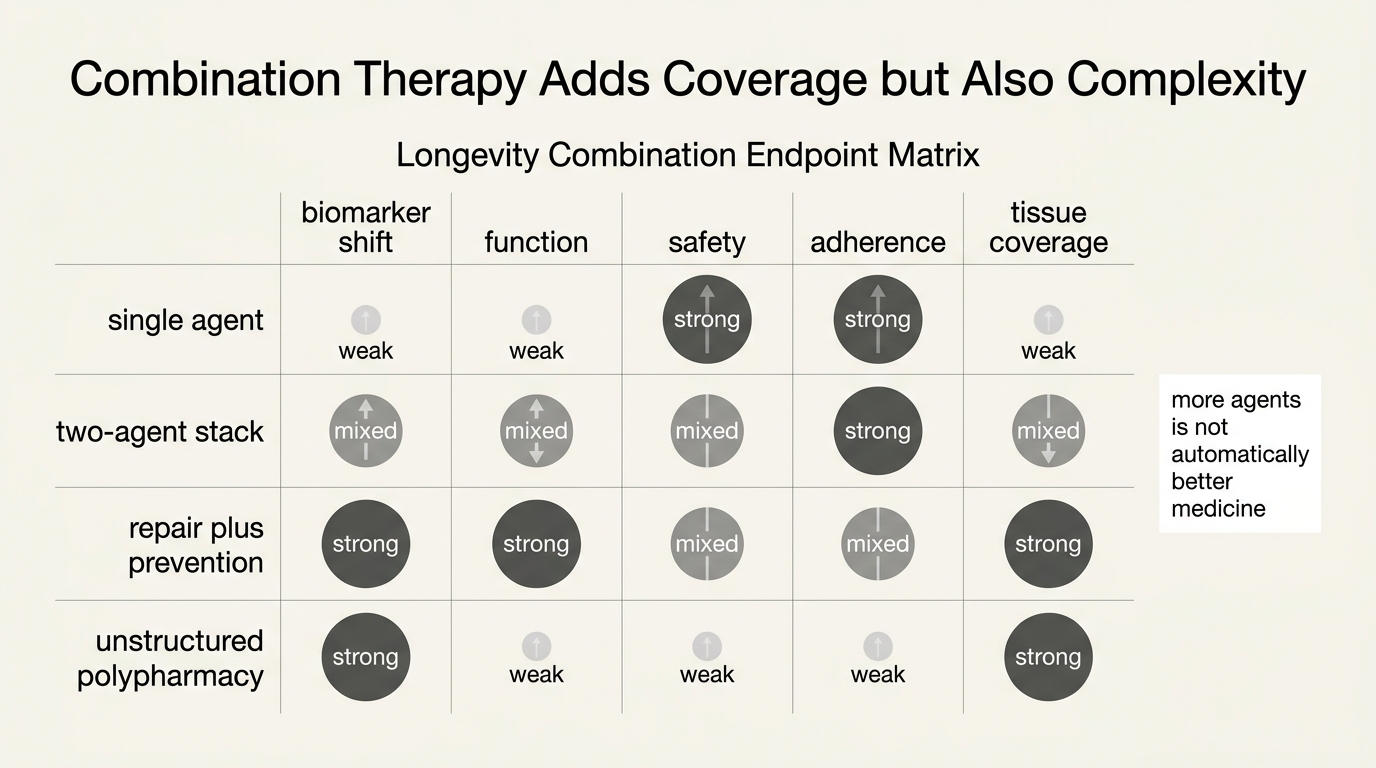
More Drugs Is Not The Same As Better Medicine
The opposite error is to assume that if one drug is incomplete, five drugs must be better. Polypharmacy without clear systems logic can create a false sense of sophistication. The goal is not maximal stacking. The goal is causal coverage with a defensible safety and monitoring plan. When the intervention list grows faster than the evidence map, the regimen starts behaving more like a speculative portfolio than a medical strategy.
That distinction matters because the longevity space already has a tendency to confuse mechanism collection with medical design. Readers should be skeptical of programs that add agents simply because each has a plausible pathway story. Plausibility is not enough. A combination should answer three questions clearly: what constraint each component addresses, what interaction risk it introduces, and which whole-person outcome justifies the extra complexity.
The Most Realistic Near-Term Path
The most realistic future is not one magic pill and not uncontrolled stacking. It is a narrower middle path: combinations tailored to phenotype, life stage, and dominant risk architecture. A metabolically unhealthy patient may benefit first from a program that improves weight, insulin sensitivity, sleep, and exercise tolerance. A frailer older patient may require a different mix oriented around muscle, inflammation control, fall prevention, and specific disease burden. That is less cinematic than a universal longevity compound, but it fits how aging actually shows up in humans.
- Expect combination logic to appear first in high-risk or clearly defined subgroups.
- Judge claims by functional endpoints, not only by biomarker breadth.
- Prefer combinations with explicit mechanistic division of labor.
- Be suspicious when regimen complexity outruns monitoring discipline.
The Standard That Matters
Single-drug approaches fail in aging for the same reason single-key explanations fail: the biology is distributed. That does not prove any given combination will work. It does set the burden of proof in the right place. The stronger longevity question is no longer whether one pathway can move. It is whether a coordinated program can change enough of the system, safely enough, to preserve human function in the real world.
Source Frame
This analysis rests on stable field structure rather than one new paper: aging is commonly modeled as a multi-process system, different tissues show different dominant failure modes, and clinical endpoint improvement often lags behind isolated biomarker movement.
What remains uncertain is which combinations will translate cleanly in humans, in what sequence they should be deployed, and how broad any eventual benefit will be outside narrower phenotypes or organ-specific use cases.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.