Compression of Morbidity vs Lifespan Extension
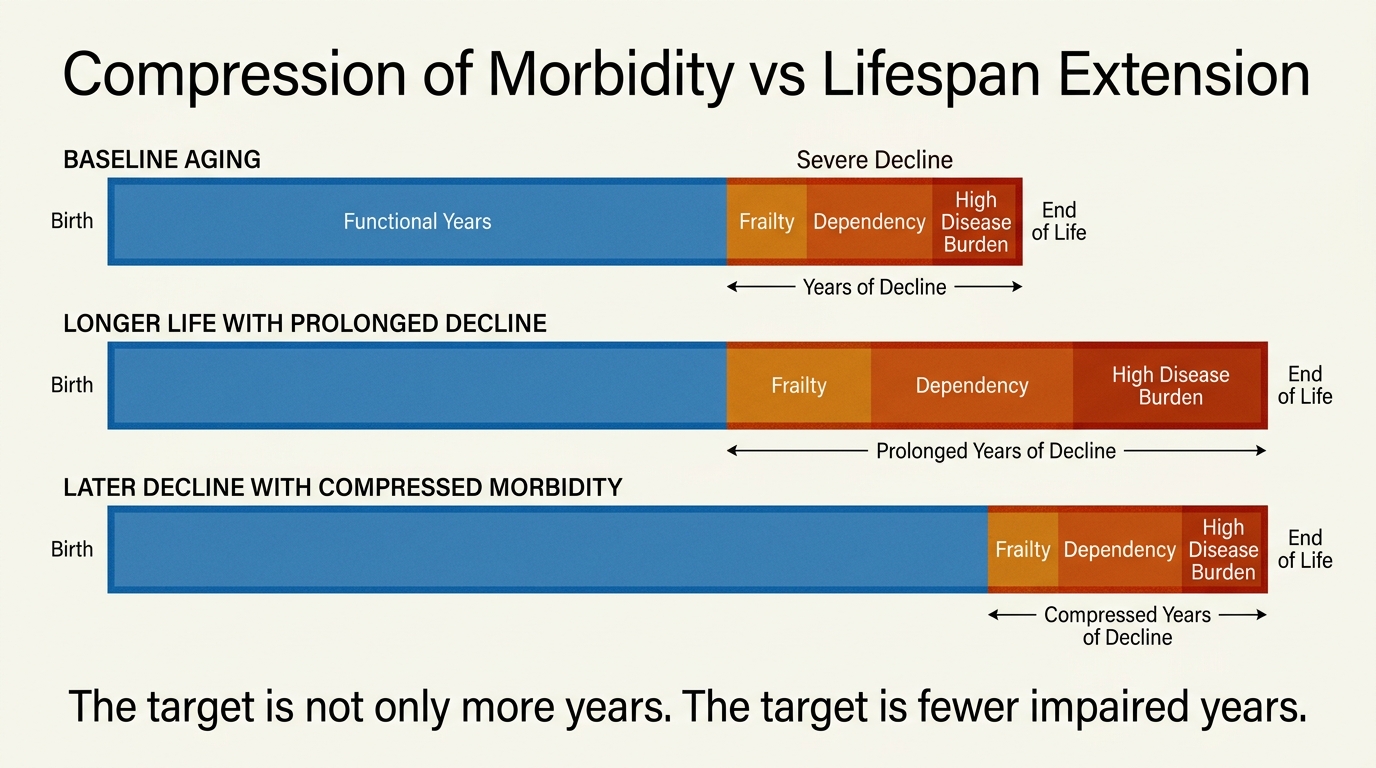
Longevity language often treats more years and better years as if they were the same outcome. They are not. A population can gain survival time while still spending a large fraction of late life in frailty, dependency, polypharmacy, and recurrent disease management. Compression of morbidity names a stricter target: keep serious functional decline concentrated into a shorter interval near the end of life rather than merely pushing death later.
That distinction matters because most real decisions in longevity medicine are not made at the level of maximum lifespan. They are made at the level of mobility, cognition, disease burden, resilience after stress, and whether one more year is lived independently or under escalating medical support. If those variables do not improve, a survival claim can still leave the core human problem unresolved.
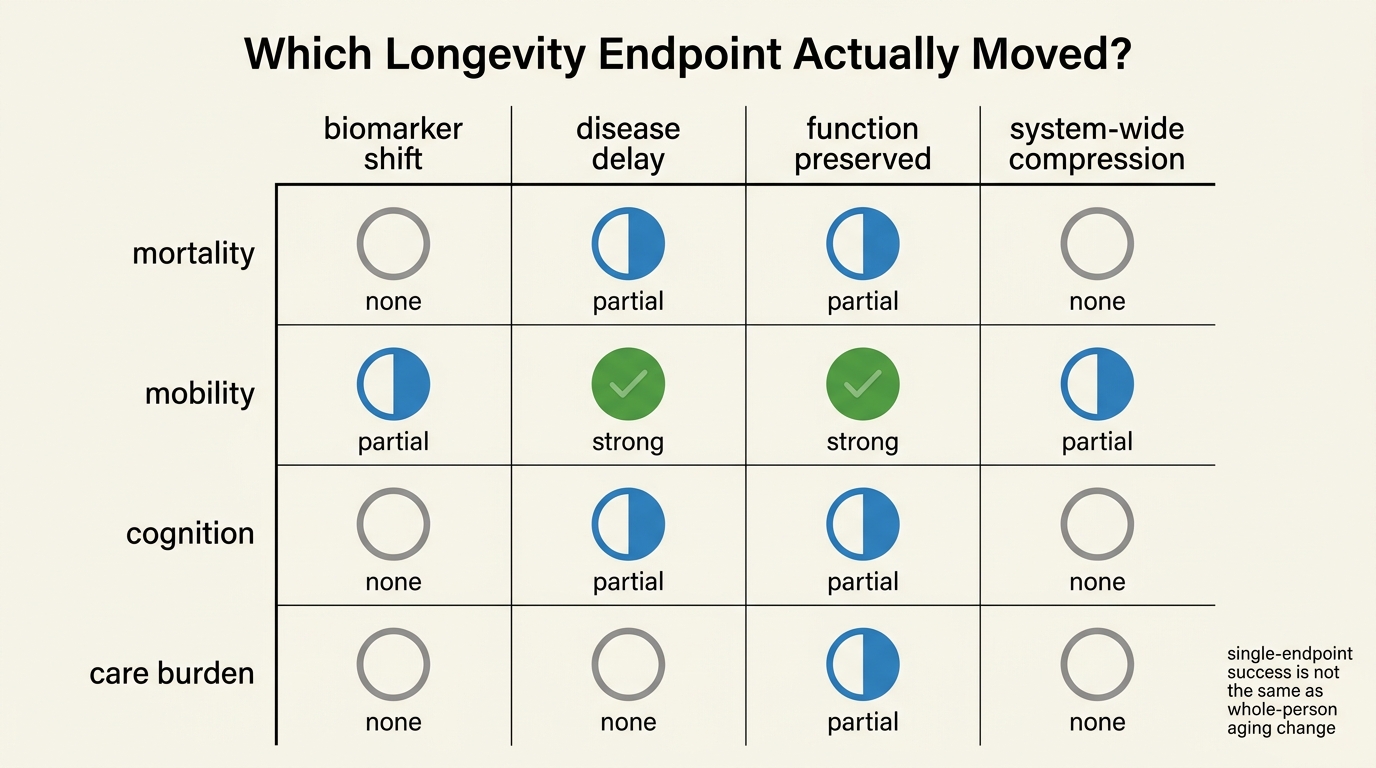
Established fact: lifespan, healthspan, disability-free survival, and disease-specific survival are different endpoints. Reasoned inference: the most useful longevity interventions are those that move more than one endpoint at once, especially by reducing the proportion of life spent in high-burden decline.
Why The Two Goals Diverge
There is no law stating that longer-lived organisms must spend the added time in good function. In animal models, some interventions lengthen lifespan by reducing specific lethal pathologies or by shifting survival under a controlled laboratory environment. That is useful biology, but it does not guarantee preserved cognition, muscle function, immune competence, or independence across the added interval. In human medicine the gap is even larger because deaths are delayed by many interacting systems, treatment cascades, and social supports.
This is why crude survival statistics can flatter weak interventions. A therapy can postpone one cause of death while leaving multimorbidity untouched. A screening regime can detect problems earlier and slightly increase measured survival from diagnosis without changing underlying degeneration. A health plan can keep patients alive longer through procedural intensity while expanding the period of chronic limitation. None of those outcomes should be confused with real rejuvenation.
What Compression Of Morbidity Actually Means
The classic concept is simple. The onset of substantial disability and high-intensity illness should occur later, and once it begins the remaining decline period should be shorter. In practical terms, that means more years with intact gait speed, strength, executive function, metabolic flexibility, and recovery capacity, followed by less time in prolonged frailty.
Compression can happen without large lifespan extension. Better blood-pressure control, smoking reduction, vaccination, fall prevention, and improvements in acute cardiovascular care have often delivered their clearest value by protecting function and reducing catastrophic events before they produce long disability arcs. That does not make them less important than dramatic life-extension stories. It makes them more relevant to actual populations.
| Endpoint | What it captures | What it misses |
|---|---|---|
| Lifespan | Total years alive | Quality, dependency, and disease burden within those years |
| Healthspan | Years with relatively preserved function | Can be defined inconsistently across studies |
| Disability-free survival | Years alive without major functional limitation | May miss subclinical decline or disease burden before disability threshold |
| Disease-specific survival | Delay of one pathology or cause of death | System-wide aging trajectory and competing causes |
Why Human Translation Is Hard
Aging is not one pathway with one clock and one endpoint. People die through different mixtures of vascular disease, cancer, neurodegeneration, sarcopenia, infection susceptibility, and loss of repair capacity. That means a signal in one biomarker, one tissue, or one model organism does not automatically tell us whether morbidity is being compressed at the whole-person level.
Measurement is another constraint. Maximum lifespan is obvious. Morbidity structure is not. Researchers need repeated functional tests, adjudicated events, frailty scores, hospitalization patterns, and long enough follow-up to see whether apparent gains are durable. Many commercial longevity claims stop far short of that bar. They lean on biomarker movement because biomarker movement is faster and cheaper to measure than years of preserved function.
How To Judge A Longevity Claim
The first question is what endpoint actually changed. If a company, clinic, or paper claims anti-aging effects, the burden is on them to specify whether they improved survival, a disease marker, a functional metric, or a composite state. Those are not semantic details. They determine whether the claim concerns true compression of morbidity or a narrower physiological effect.
The second question is whether the gain is systemic or local. For example, improved glucose control may reduce one risk channel while leaving neurodegeneration, muscle loss, and immune decline largely untouched. That can still be worthwhile, but the interpretation should be narrow. Compression of morbidity requires broader coordination across the failure modes that make late life medically expensive and personally constraining.
- Ask whether function improved, not only whether a biomarker moved.
- Ask whether the intervention reduces multi-system burden or one isolated risk factor.
- Ask whether the added time is independent, mobile, and cognitively intact.
- Ask whether adverse effects offset the apparent longevity gain.
Why Compression May Be The Better Near-Term Target
For translational medicine, compression of morbidity is often a more realistic and ethically cleaner target than dramatic lifespan extension. Preserving function, delaying frailty, and reducing years of severe dependency can be measured sooner and matter immediately to patients. They also align better with healthcare economics, caregiver burden, and quality of life than survival extension divorced from capability.
This does not make lifespan extension irrelevant. If an intervention extends both life and function, that is stronger evidence of meaningful aging modification. The point is that the order of proof should be disciplined. A credible program should first show that people are aging into better late-life states, not simply into longer treatment histories.
The Strongest Longevity Standard
The rigorous benchmark is neither pure lifespan nor vague wellness. It is a package: later onset of chronic dysfunction, better reserve while stress accumulates, fewer years under heavy disability, and no major tradeoff in cancer risk, cognitive decline, or treatment burden. That is a demanding standard, but it is closer to the real human objective than celebratory language about adding years in abstraction.
Compression of morbidity therefore acts as a filter against weak inference. It forces researchers, clinics, and readers to ask whether a longevity story changes the shape of aging or only one visible segment of it. That shift in framing matters because medicine has many ways to prolong late-life management. It has far fewer ways to preserve a life that remains recognizably capable.
Source Frame
This analysis rests on established distinctions used across epidemiology, geriatrics, survival analysis, and geroscience: lifespan versus healthspan, disease-specific outcomes versus whole-person function, and frailty or disability trajectories as separate endpoints from mortality alone.
What remains uncertain is how often any current longevity intervention in humans produces true multi-system compression of morbidity rather than narrower risk reduction. That is still an open empirical question for most proposed therapies.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.