Tissue Engineering for Age-Related Degeneration
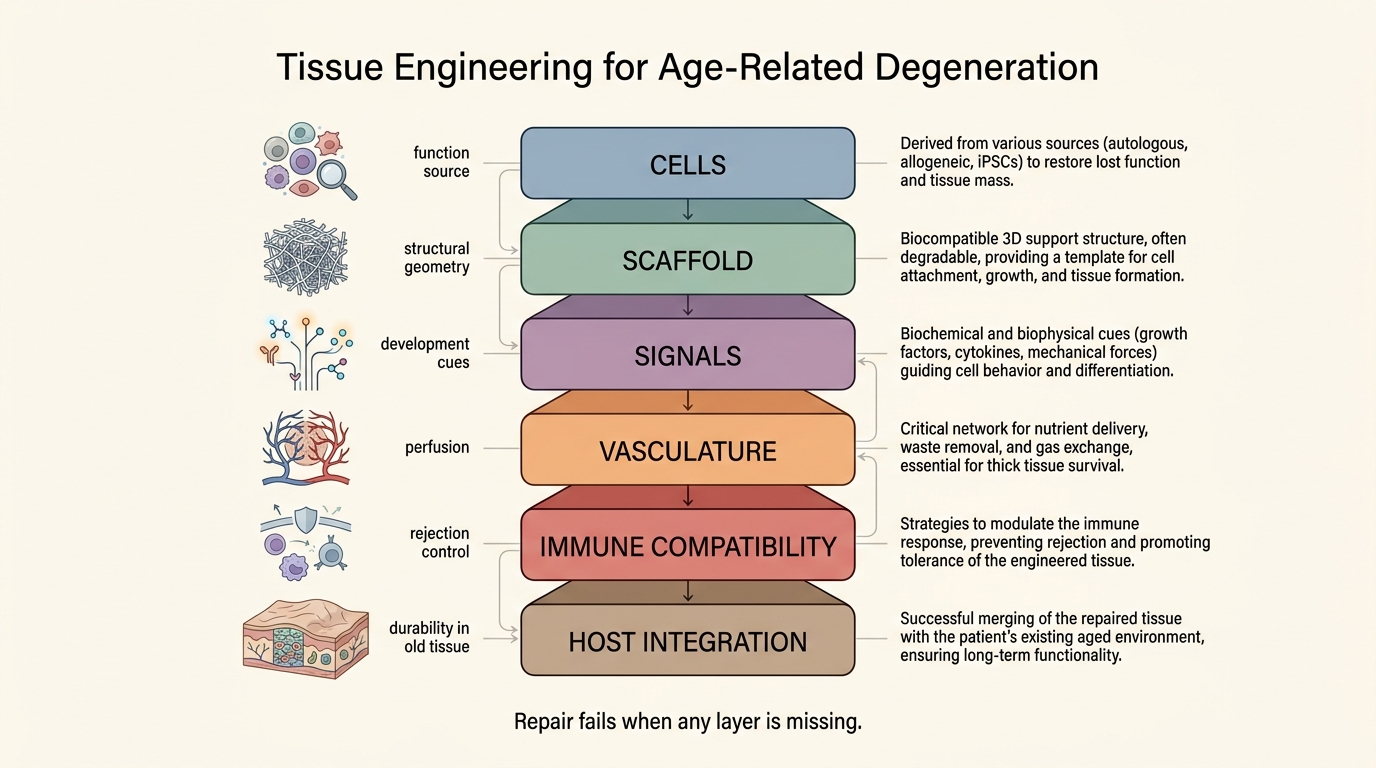
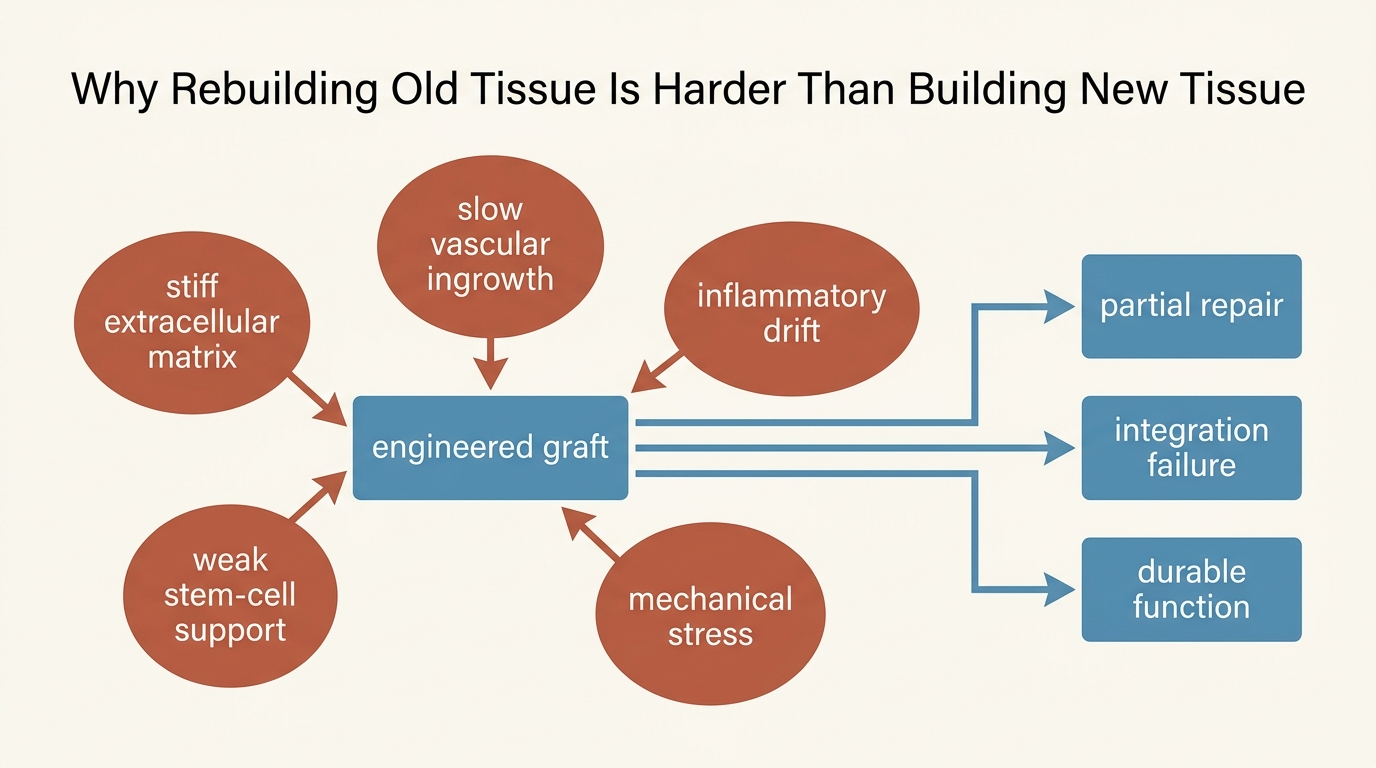
Most age-related degeneration is described as if one component failed and one replacement technology merely needs to arrive. Real tissue decline is not that tidy. Cells lose function, extracellular matrix stiffens, vasculature thins, immune signaling drifts, and the surrounding mechanical environment becomes less permissive to repair. Tissue engineering matters because it tries to rebuild structure rather than only modulate pathways. It remains hard because old tissues fail as systems, not as isolated parts.
The strongest version of the field is already real. Engineered matrices, skin substitutes, graft materials, and scaffold-guided repair strategies have shown that biological structure can be rebuilt in bounded settings. The weaker but popular version is that the same logic can soon replace or rejuvenate aged organs wholesale. That second claim is still much less mature. The central obstacle is not imagination. It is integration.
Core thesis: tissue engineering is a credible repair technology for selected age-related degenerative problems, but its translational ceiling is set by vascularization, immune compatibility, innervation, mechanical durability, and the aged host environment. The established fact is that engineered tissue can work in narrower repair domains. The inference, often overstated, is that organ-scale rejuvenation is therefore near.
Why Degeneration Is A Structural Problem
Aging tissues rarely fail for one reason. Cartilage degeneration is not only cell depletion. Skeletal muscle decline is not only satellite-cell exhaustion. Skin thinning is not only collagen loss. Organ aging usually combines altered matrix architecture, senescent-cell burden, chronic inflammatory signaling, weaker stem-cell function, and slower vascular response. That is why purely pharmacologic interventions often produce incomplete repair. They may reduce one driver while leaving the damaged substrate in place.
Tissue engineering enters at precisely that point. It treats the damaged substrate as part of the disease. That makes it more ambitious than a signaling-only intervention and often more biologically coherent. An engineered scaffold can restore geometry. A cell-loaded construct can reintroduce missing function. A bioreactor-grown graft can be preconditioned before implantation. The field has therefore moved beyond the old caricature that it is merely speculative lab craft.
Still, the field is not operating against fresh tissue. It is usually entering an old host. That old host has impaired angiogenesis, altered immune tone, fibrosis, slower integration, and weaker regenerative reserve. The engineered construct is therefore asked to perform inside the very environment that caused degeneration in the first place.
Where The Field Already Has Real Strength
The strongest current evidence is not whole-organ replacement for routine aging. It is bounded reconstruction. Skin repair, scaffold-assisted wound healing, cartilage and bone reconstruction, corneal and airway work, and some decellularized-matrix applications show that structure-aware regenerative medicine can solve problems that drugs alone do not solve cleanly. Those successes matter because they prove the governing principle: biological architecture can be designed and therapeutically useful.
They do not automatically imply that brain, kidney, heart, or liver aging can be reversed by extending the same recipe. Organ-scale aging brings density, perfusion, electrical coordination, immune exposure, and long-run durability constraints that are much harder than repairing a thinner, more accessible tissue plane.
This is the first discipline readers need. A clinically meaningful repair technology in one tissue class is still a meaningful advance. It does not need to be a whole-body rejuvenation platform to count.
The Old-Environment Problem
Regeneration headlines often focus on the graft or construct itself. For aging, the host environment is equally important. An old extracellular matrix can distort cell behavior even when the cells are competent. Aged vasculature may delay perfusion of implanted tissue. Low-grade inflammation can disrupt engraftment. Immune surveillance can become both weaker and more dysregulated. A tissue-engineered solution that performs well in a younger model may therefore degrade sharply in an older body.
This is why the topic belongs next to extracellular matrix aging, stem-cell exhaustion, and tissue-specific senescence. Tissue engineering is not a separate miracle lane. It is a convergence problem that inherits the weaknesses of every aged component it depends on.
Replacement Is Not Rejuvenation
One of the most common confusions in this space is the collapse of replacement into rejuvenation. A replaced surface, patch, conduit, or segment can be therapeutically valuable without proving that systemic aging has been slowed. The distinction matters because many age-related degenerative conditions will likely be managed through local repair tools before any broad anti-aging claim becomes justified.
That is not a disappointment. It is probably the realistic path. Aging medicine may advance through a stack of organ- and tissue-level interventions that restore function in specific places rather than through one universal reset. Tissue engineering fits that model well. It can meaningfully improve mobility, wound healing, structural integrity, and local tissue function even if it does not solve whole-organism aging.
The stronger rejuvenation claim would require something broader: durable restoration of aged tissue behavior, not only replacement of a damaged piece. That pushes the field toward vascular engineering, immune programming, better biomaterials, and possibly combinations with partial reprogramming or other state-reset technologies. Those combinations are conceptually interesting. They are also much less validated.
What Translation Still Needs
- Perfusion at useful scale. Thick tissues need rapid vascular integration or prebuilt vascular networks. Diffusion alone is not enough.
- Mechanical fit. A graft that survives implantation but fails under real stress has not solved degeneration.
- Immune governance. Tolerance, inflammation control, and infection risk still shape outcomes as much as cell selection.
- Manufacturing consistency. Aging medicine cannot rely on artisanal constructs if the goal is broad clinical use.
- Evidence that matters to old patients. Functional restoration, durability, and complication rates matter more than elegant short-term images.
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | Tissue engineering and regenerative-medicine platforms have produced clinically useful repair tools in selected tissues and reconstructive settings. |
| Known | Age-related degeneration usually involves multiple coupled failures, including matrix change, vascular decline, inflammatory drift, and weaker cell-state maintenance. |
| Known | Unapproved regenerative-medicine claims remain a real safety problem, and FDA has repeatedly warned against broad clinic marketing that outruns evidence. |
| Inferred | The most durable near-term value of tissue engineering in aging will likely come from local structural repair and disease-specific reconstruction rather than from whole-organ rejuvenation. |
| Inferred | Combination approaches that improve the aged host environment may matter as much as improvements in the engineered construct itself. |
| Unknown | Which organ systems will first show durable, scalable, age-specific benefit once vascularization, manufacturing, and immune-integration hurdles are tested in larger human programs. |
Practical Reading For LifeMeter
The practical implication is not to dismiss the field and not to mythologize it. Tissue engineering is one of the few domains that directly addresses the structural dimension of aging. That gives it real strategic importance. It also means the proof burden is unusually high. A claim of true repair should be asked to show function, integration, and durability inside older tissue, not only elegant construct design in a controlled setting.
Readers should therefore treat the field as a serious repair stack with uneven maturity. Skin, musculoskeletal, wound, and bounded reconstructive use cases can advance meaningfully before heart, kidney, or brain regeneration is routine. That staggered path is not evidence of failure. It is what honest translation usually looks like.
Source List
Langer R, Vacanti JP. Tissue Engineering. Science. 1993.
Annabi N, Cosgriff-Hernandez E, Weiss AS, et al. Perspectives on Recent Developments and Directions in Tissue Engineering and Regenerative Medicine. Tissue Engineering Part A. 2024.
Foundational literature on decellularized matrices, scaffold-guided repair, organoid and bioprinting systems, and vascularization bottlenecks in regenerative medicine.
U.S. Food and Drug Administration. Consumer Alert on Regenerative Medicine Products Including Stem Cells and Exosomes. Updated July 22, 2020.
U.S. Food and Drug Administration. Important Patient and Consumer Information About Regenerative Medicine Therapies. Updated June 3, 2021.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.