Insulin Sensitivity as a Longevity Lever
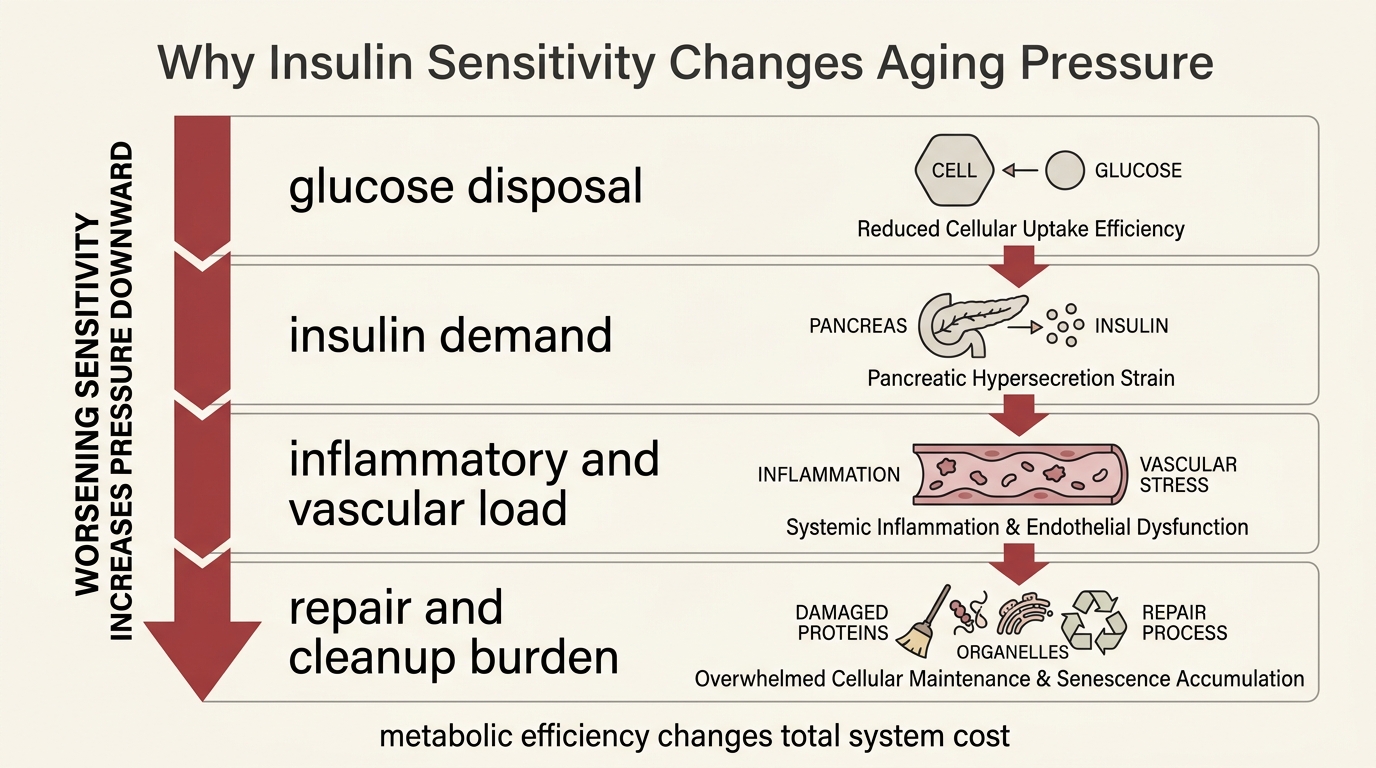
The body can tolerate high glucose only by paying for it elsewhere. When insulin sensitivity falls, more hormone is required to move the same fuel. That extra metabolic pressure spills into adiposity, vascular strain, inflammatory tone, and impaired cellular cleanup long before a diabetes diagnosis makes the problem obvious.
This is why insulin sensitivity matters to longevity even though it is not itself a lifespan guarantee. It changes how hard the organism has to work to maintain glucose control. It changes how much insulin circulates for how long. It changes whether energy excess is stored cleanly, burned flexibly, or converted into a chronic stress signal that other tissues keep paying for.
Core thesis: insulin sensitivity is a real longevity lever because it reduces metabolic overdrive and downstream disease risk, but the strongest case is still healthspan architecture rather than a single direct human lifespan proof.
Why This Matters Beyond Diabetes
Insulin sensitivity is often discussed as a prediabetes variable. That framing is too narrow. The broader issue is metabolic cost. A system that needs more insulin to achieve the same glucose disposal is already operating under worse terms. Hyperinsulinemia can coexist with normal fasting glucose for years, which is why apparently stable labs can still hide a progressively more expensive control regime.
That cost matters because insulin is not only a glucose-lowering hormone. It also influences nutrient storage, lipogenesis, endothelial function, and signaling pathways tied to growth and repair. When insulin remains chronically elevated, the body is not merely correcting glucose. It is living inside a more anabolic, less flexible operating state. That makes this topic belong next to metformin, ketones, and amino acid restriction rather than inside diabetes management alone.
The Longevity Signal Is Stronger In Mechanism Than In Direct Human Lifespan Data
The mechanistic case is substantial. Across model organisms and several mouse longevity paradigms, lower insulin signaling or preserved insulin sensitivity often tracks with longer life or slower physiological deterioration. That does not transfer cleanly into a simple human rule, because insulin biology in humans is entangled with adiposity, muscle mass, diet quality, medication use, and disease status.
The careful interpretation is narrower. Human populations with preserved insulin sensitivity tend to show better cardiometabolic aging profiles and lower burden from the diseases that usually cut healthspan first. That is meaningful. It still does not prove that raising insulin sensitivity in any one person will automatically extend lifespan, because intervention quality, tissue context, and the cause of the resistance all matter.
Hyperinsulinemia Creates A Repair Problem, Not Only A Fuel Problem
Once insulin resistance develops, the pancreas often compensates by secreting more insulin. That compensation protects glucose control for a while, but it also keeps more of the system exposed to elevated anabolic signaling. Reviews of insulin and aging keep returning to the same concern: chronically high insulin can support lipogenesis, interact with mTOR signaling, and weaken autophagic housekeeping in ways that look aging-relevant even before overt disease appears.
This does not mean insulin is harmful by nature. It means the balance matters. Insulin is essential to life. The issue is prolonged overuse inside a system that has become resistant to its own controller. Longevity readers should therefore treat insulin sensitivity as an efficiency question. How much hormonal force is required to keep basic energy regulation working, and what collateral burden does that create elsewhere?
| Layer | Why it matters for aging | Common mistake |
|---|---|---|
| Glucose control | Reduces glycemic volatility and downstream vascular damage | Treating normal glucose as proof that the system is low-stress |
| Hormonal demand | Lowers the amount of insulin required to maintain control | Ignoring hyperinsulinemia because fasting glucose still looks acceptable |
| Metabolic flexibility | Improves the ability to shift between storage and fuel use | Assuming all weight loss or all carbohydrate restriction creates the same effect |
| Repair environment | May reduce signaling patterns linked to lipogenesis, inflammation, and impaired cleanup | Claiming that one metabolic marker alone proves slowed aging |
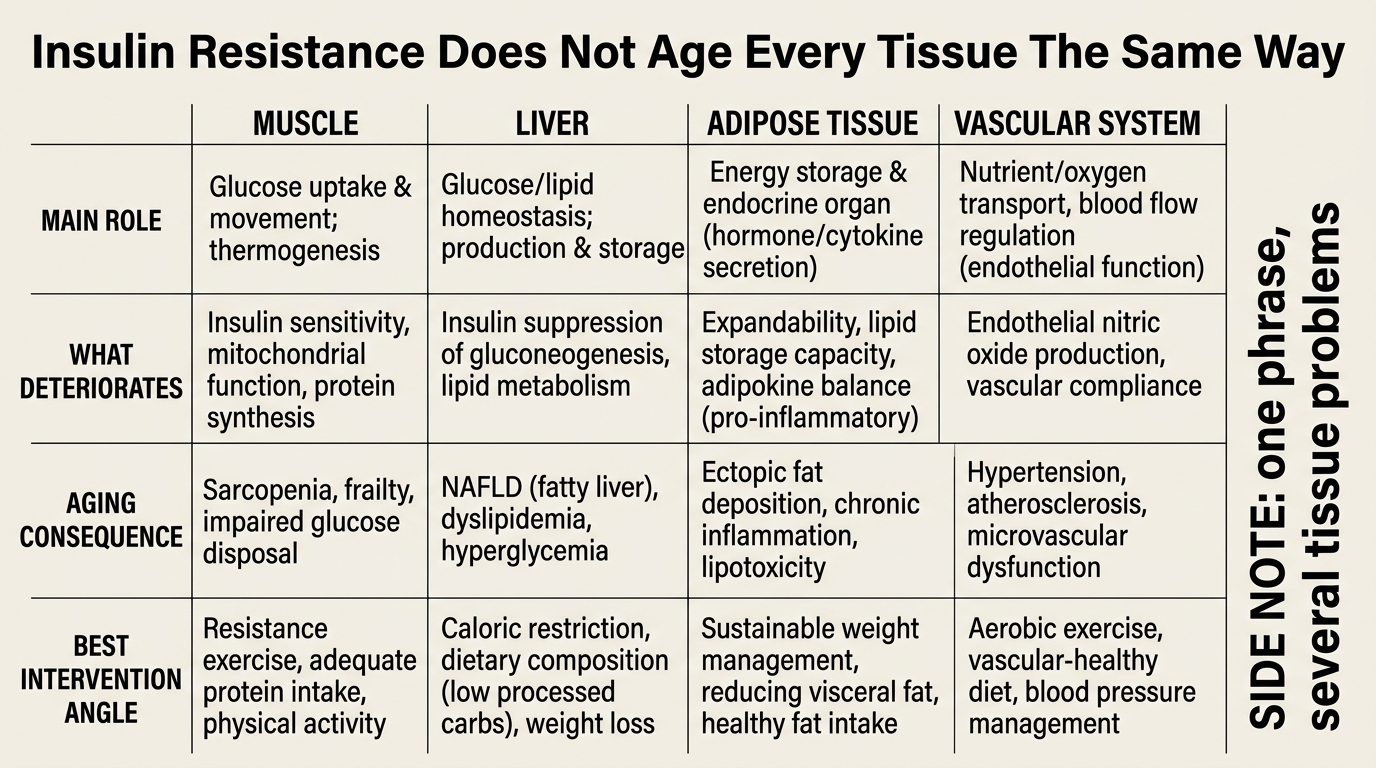
Muscle, Liver, And Adipose Tissue Do Not Age The Same Way
One reason insulin-sensitivity stories become sloppy is that the term sounds singular. In practice, tissues diverge. Skeletal muscle determines a large share of postprandial glucose disposal. Liver insulin resistance reshapes glucose output and triglyceride handling. Adipose dysfunction changes free-fatty-acid flux, inflammatory signaling, and how safely energy can be buffered. A person can therefore improve one layer and still leave another poorly controlled.
This is why body composition, physical activity, sleep, and adipose distribution matter so much. The useful goal is not a purity narrative about one diet or one supplement. It is a better tissue environment. Exercise improves insulin action through routes that go beyond weight alone. Fat loss often helps, but the location and physiology of fat mass matter. Drug effects can be real, but they inherit the same tissue-specific limits.
What A Decision-Grade Longevity Take Looks Like
A decision-grade interpretation keeps three ideas separate. First, preserved insulin sensitivity is good because it lowers disease pressure and metabolic cost. Second, the largest benefits probably come from the basics that alter tissue physiology broadly: movement, body-composition quality, sleep, and food environments that reduce chronic overfeeding. Third, no serious reader should confuse those points with proof that insulin sensitivity is the sole driver of human aging.
The practical implication is stronger than motivational advice and weaker than miracle language. Readers should not wait for a geroscience endpoint to care about this variable. They should also not overstate it as the entire longevity map. Insulin sensitivity is one of the best examples of a lever that is both genuinely important and frequently oversold.
- Watch fasting insulin, glucose tolerance, waist change, and training capacity together rather than treating one marker as the whole story.
- Favor interventions that improve tissue function and adherence, not only short-term glucose optics.
- Read drug-based improvements through muscle, liver, and adipose tradeoffs instead of assuming a universal anti-aging effect.
- Use insulin sensitivity as a systems-health signal, not as a standalone substitute for broader longevity measurement.
Known, Inferred, And Unknown
| Category | Assessment |
|---|---|
| Known | Insulin resistance and hyperinsulinemia are associated with higher risk of type 2 diabetes, cardiovascular disease, fatty liver disease, and other age-related disorders that compress healthspan. |
| Known | Animal longevity models frequently show a relationship between reduced insulin signaling or preserved insulin sensitivity and longer lifespan or improved late-life physiology. |
| Known | Exercise, weight reduction in the right context, sleep improvement, and selected medications can improve insulin sensitivity in humans, though effect size and durability vary widely. |
| Inferred | Part of the longevity value of insulin sensitivity likely comes from lowering chronic anabolic stress and preserving cellular housekeeping rather than from glucose control alone. |
| Unknown | Which intervention sequences produce the largest long-run human longevity benefit once insulin sensitivity, muscle preservation, adherence, and medication tradeoffs are all priced together. |
Source Frame
This analysis draws on the mouse and endocrine-aging literature linking insulin signaling to lifespan structure, including Masternak et al. on insulin sensitivity and longevity mechanisms.
For the human caution layer, it relies on the broader review frame in Kolb, Kempf, and Martin on insulin and aging, which argues that the healthspan signal is real while direct anti-aging simplifications remain weak.
The unresolved question is not whether insulin sensitivity matters. It is how much of its longevity value comes from lowering disease incidence, how much comes from reducing deeper repair burden, and which interventions can improve it without creating new tradeoffs elsewhere.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.