Organ Replacement vs Organ Rejuvenation
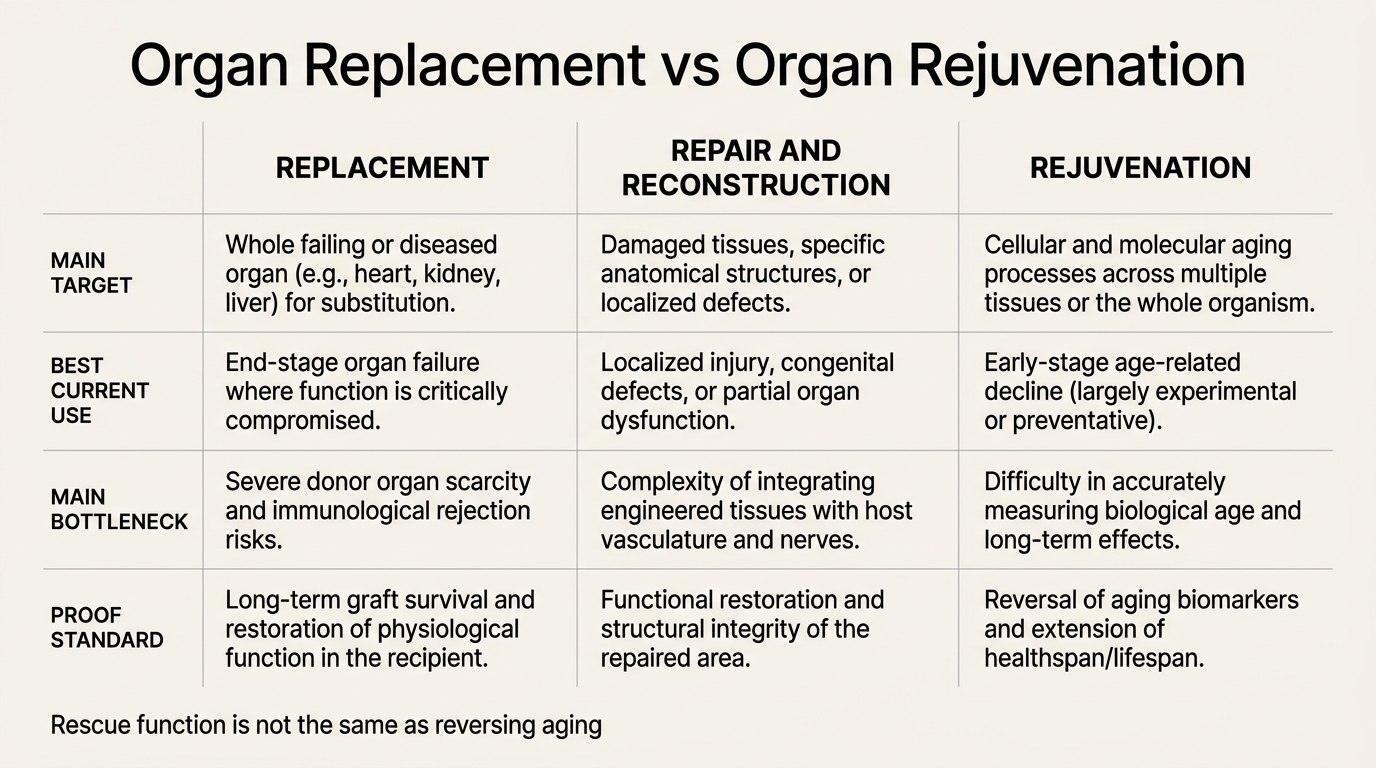
Organ replacement and organ rejuvenation are often compressed into one futuristic promise. They are not the same strategy. Replacement solves organ failure by swapping, reconstructing, or mechanically supporting damaged tissue. Rejuvenation aims to make an old biological system behave younger again, including the tissue environment that made organ failure likely in the first place.
The distinction matters because replacement already works in bounded settings. Kidney, liver, heart, lung, and corneal transplantation save lives. Tissue engineering can patch cartilage, skin, airway, and wound problems under some conditions. None of that means medicine has solved systemic aging. A transplanted or engineered organ still has to survive inside an older host with inflammatory tone, vascular wear, immune exposure, matrix damage, and repair limits that the replacement itself does not erase.
Established fact: organ replacement and ex vivo organ support have advanced meaningfully through transplantation, machine perfusion, and targeted tissue engineering. Reasoned inference: those advances improve rescue and repair more directly than they solve whole-body aging, because host biology remains the governing constraint once the graft enters an older system.
What Replacement Already Does Well
Replacement has a narrow and serious logic. If an organ has failed past the point of intrinsic recovery, the fastest path back to function may be to transplant a new organ, implant a durable assist device, or reconstruct the damaged tissue architecture directly. That logic is concrete, which is why transplantation medicine built real outcome gains long before anti-aging medicine existed as a category.
The same bounded logic explains why tissue engineering is strongest in anatomically tractable problems. Localized repair with clear structural targets tends to outperform diffuse systemic regeneration. Skin, cornea, cartilage, vascular grafts, and scaffold-mediated reconstruction work better than whole-organ fabrication because the geometry, perfusion, and integration problem is still within reach.
Why Rejuvenation Is a Different Claim
Rejuvenation is not mainly about rescue from terminal organ failure. It is about altering the aged state itself. That means addressing damage accumulation, stem-cell depletion, matrix change, inflammatory dysregulation, mitochondrial decline, and the signaling environment that makes older tissues harder to repair cleanly. A rejuvenated kidney is not merely a kidney transplant outcome. It is the claim that an older kidney or its surrounding host can be pushed toward younger function without replacing the entire unit.
That makes the proof burden higher. Replacement can be judged by graft function, rejection rates, ischemia time, and survival. Rejuvenation has to show that tissue quality, repair capacity, and system-level biology improved in a way that is durable and not canceled by tradeoffs such as malignancy risk, fibrosis, immune drift, or unstable cell identity.
| Question | Replacement frame | Rejuvenation frame |
|---|---|---|
| Main target | Failed organ or damaged tissue segment | Aged cellular and tissue state |
| Clinical objective | Restore function after failure or structural loss | Recover youthful repair capacity before or after decline |
| Primary bottleneck | Supply, immune fit, ischemic injury, surgical durability | Host environment, cell-state control, systemic aging burden |
| Current maturity | Established in transplant medicine, limited in organ fabrication | Earlier, uneven, and mostly bounded to partial repair concepts |
The Older Host Is the Hidden Variable
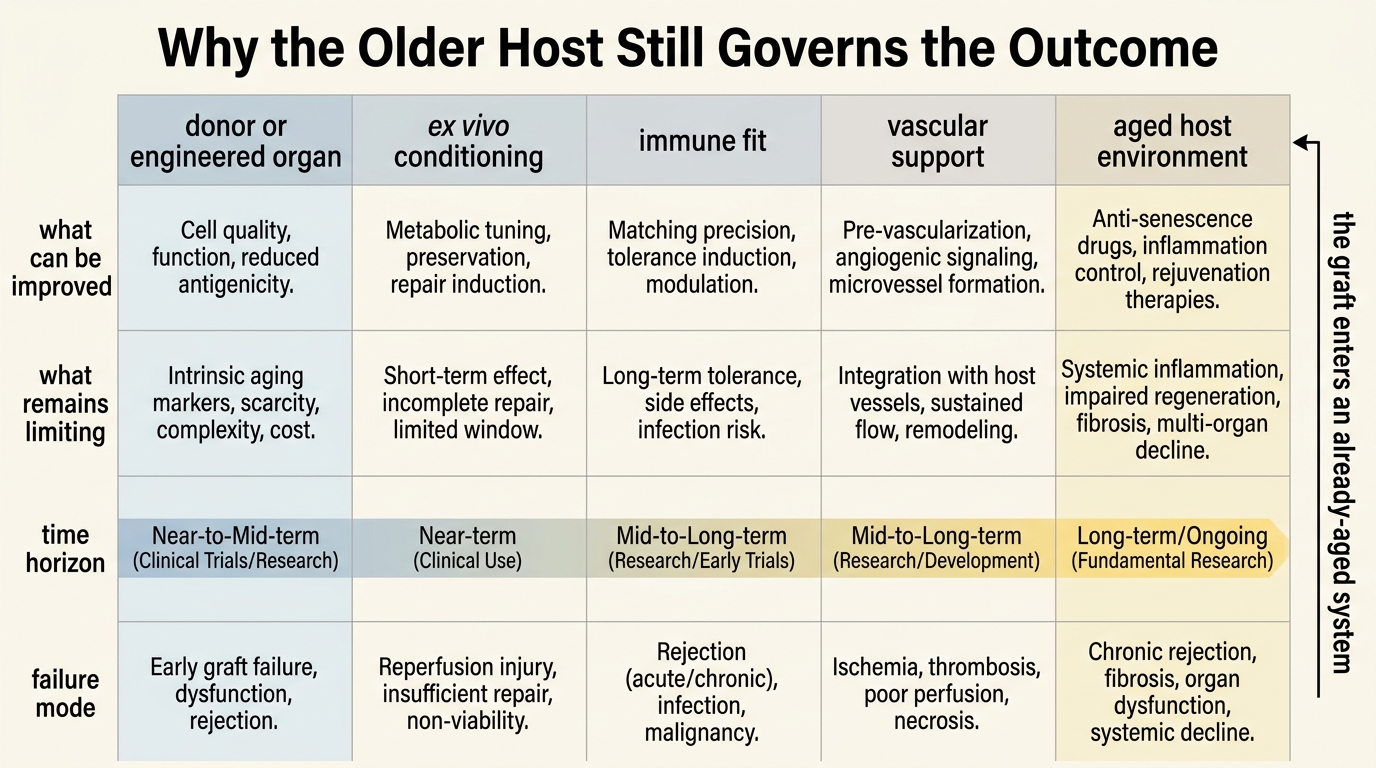
This is where optimistic narratives usually blur. A graft can be technically successful while the host remains biologically old. That matters because older recipients often bring immunosenescence, vascular disease, fibrosis, chronic inflammation, and weaker regenerative coordination into the postoperative environment. The organ problem and the host problem are related but distinct.
Even ex vivo organ conditioning, which is one of the most promising bridges between replacement and rejuvenation, operates inside that limit. Machine perfusion can extend preservation windows, evaluate donor quality, and create a temporary platform for repair or gene-delivery strategies outside the body. Once the organ is implanted, however, it still has to survive the recipient milieu. That is why ex vivo repair is exciting but not equivalent to solving aging.
Where the Boundary Is Most Productive
The best current frontier is not choosing replacement or rejuvenation as rival doctrines. It is using each where it has real leverage. Organ support, ex vivo conditioning, scaffold repair, and cell-based reconstruction can buy function. Rejuvenation research can then ask whether the recipient tissue environment can be made more permissive, less inflammatory, and less fibrotic so that repairs last longer and fail less often.
That combined view fits the rest of the regenerative pillar. Stem-cell reserve, matrix quality, and systemic environment all change whether a repaired structure remains functional. The field is strongest when it treats organ rescue and host rejuvenation as linked but non-identical layers.
Whole-Organ Fabrication Still Faces a Physics Problem
Most whole-organ regeneration claims encounter the same set of barriers: vascularization, innervation, immune compatibility, architecture at multiple scales, and stable integration into living circulation. These are not branding problems. They are engineering and developmental-biology problems. Any article that treats them as a short timeline issue is overstating the maturity of the field.
This does not weaken the replacement case. It narrows it. Organ fabrication remains a frontier project. Organ support, organ preservation, and partial tissue reconstruction are the domains that already matter clinically. Readers should therefore separate current transplant and tissue-engineering progress from the stronger narrative that organ-scale rejuvenation is close to routine deployment.
Decision-Grade Take for Longevity Readers
Longevity readers should treat organ replacement as rescue medicine with important translational spillovers, not as the direct endpoint of anti-aging strategy. It extends life in some settings because it restores indispensable function. It does not by itself reverse the aged state of the person receiving the organ.
- Read transplant and tissue-engineering progress as evidence that structural repair can work under bounded conditions.
- Do not infer from graft survival that the host has been rejuvenated.
- Track ex vivo organ conditioning as a serious bridge technology because it may improve repair quality before implantation.
- Keep the main proof burden on whether repaired tissues stay durable inside older biological environments.
Known, Inferred, and Unknown
| Category | Assessment |
|---|---|
| Known | Solid-organ transplantation and targeted tissue repair already restore function in many forms of end-stage organ failure or localized degeneration. |
| Known | Ex vivo machine perfusion can improve organ preservation, organ assessment, and opportunities for organ reconditioning before transplantation. |
| Known | Older host biology changes repair outcomes through immune status, vascular quality, fibrosis, and broader systemic aging effects. |
| Inferred | The strongest near-term gains may come from combining replacement or reconstruction with therapies that improve host repair conditions rather than expecting replacement alone to solve the aging problem. |
| Unknown | Which interventions can reliably make older recipients biologically permissive enough that repaired or engineered organs behave as though they entered a younger host. |
Source Frame
This analysis relies on the regenerative-medicine distinction between replacement and true regeneration outlined in Rando and Chang on rejuvenation as an integrated regenerative strategy.
For the transplant-host constraint, it uses Slegtenhorst and colleagues on injury and repair in older organ transplants, which emphasizes that aging changes how transplanted organs tolerate stress and recover.
For the bridge technology layer, it draws on the review of ex vivo gene therapy and machine perfusion in organ transplantation and the broader recent discussion in Anti-aging strategies and ex vivo organ rejuvenation. The open question is not whether replacement works. It is how much of the remaining aging burden can be shifted from rescue toward durable rejuvenation.
Translate this longevity claim into a capital-runway decision.
Life extension logic only matters if the balance sheet can carry it. Move into WealthMeter to compare assets, spending, and yield assumptions against the same long-horizon planning problem.